Article Text

Abstract
Background Available evidence on the comparative efficacy and acceptability of psychotherapies for post-traumatic stress disorder (PTSD) in children and adolescents remains uncertain.
Objective We aimed to compare and rank the different types and formats of psychotherapies for PTSD in children and adolescents.
Methods We searched eight databases and other international registers up to 31 December 2020. The pairwise meta-analyses and frequentist network meta-analyses estimated pooled standardised mean differences (SMDs) and ORs with random-effects model. Efficacy at post-treatment and follow-up, acceptability, depressive and anxiety symptoms were measured.
Findings We included 56 randomised controlled trials with 5327 patients comparing 14 different types of psychotherapies and 3 control conditions. For efficacy, cognitive processing therapy (CPT), behavioural therapy (BT), individual trauma-focused cognitive–behavioural therapy (TF-CBT), eye movement desensitisation and reprocessing, and group TF-CBT were significantly superior to all control conditions at post-treatment and follow-up (SMDs between −2.42 and −0.25). Moreover, CPT, BT and individual TF-CBT were more effective than supportive therapy (SMDs between −1.92 and −0.49). Results for depressive and anxiety symptoms were similar to the findings for the primary outcome. Most of the results were rated as ‘moderate’ to ‘very low’ in terms of confidence of evidence.
Conclusions CPT, BT and individual TF-CBT appear to be the best choices of psychotherapy for PTSD in young patients. Other types and different ways of delivering psychological treatment can be alternative options. Clinicians should consider the importance of each outcome and the patients’ preferences in real clinical practice.
- child & adolescent psychiatry
Data availability statement
Data are available in a public, open access repository. With the publication of this article, the full dataset will be freely available online in Mendeley Data, a secure online repository for research data, which allows archiving of any file type and assigns a permanent and unique digital object identifier (DOI) so that the files can be easily referenced (DOI: 10.17632/278y88n8r7.1).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Post-traumatic stress disorder (PTSD) is a common and severe psychological disorder in children and adolescents.1 About 30%–60% of young people who have experienced traumatic events can develop PTSD.2 Types of traumatic events that may cause PTSD in children and adolescents mainly include physical or sexual abuse, war or terrorism, natural or man-made disasters, catastrophic illnesses and accidents.3 Additionally, prolonged, repeated experience of trauma in a context in which the individual has little or no chance of escape may cause complex PTSD.4 Compared with adults, children and adolescents with PTSD reported higher levels of anxiety and depression, and lower levels of optimal functioning in different settings (eg, at home and school).5 Moreover, untreated PTSD is a key determinant for poor health outcomes, such as elevated risk of psychiatric disorders or suicidality, highlighting the importance of identifying and addressing psychological needs of traumatised minors.6
Currently, psychotherapies are recommended as the first-line treatment of PTSD in children and adolescents according to several international guidelines, and various forms of psychotherapies such as trauma-focused cognitive–behavioural therapy (TF-CBT) and eye movement desensitisation and reprocessing (EMDR) are commonly used.7 8 Previous pairwise meta-analyses found evidence to support the effectiveness of psychotherapies in reducing PTSD, anxiety and depression symptoms.9 10 However, these studies were inconclusive because they were not able to generate clear hierarchies among available interventions, due to many psychotherapies that have not been directly compared. Moreover, the debate regarding whether the inclusion of a trauma-focused component (eg, exposure to traumatic memories) is essential in CBT11 and whether the effectiveness of psychotherapy delivered individually or in group format is different for children and adolescents with PTSD is still ongoing.12 These issues make decision-making uncertain for healthcare professionals and patients.13 14
Objective
In this study, we aimed to synthesise, compare and rank all the available evidence on commonly used psychotherapies for the treatment of PTSD in children and adolescents.
Methods
Search strategy and selection criteria
We performed a comprehensive literature search for published and unpublished randomised controlled trials (RCTs) in PubMed, Cochrane Central Register of Controlled Trials, Embase, Web of Science, PsycINFO, CINAHL, PILOTS, ProQuest Dissertations, international trial registers from inception until 31 December 2020 (online supplemental appendix 1). Eligible trials included comparisons of any manualised or structured psychotherapy with another psychotherapy or any control condition for the treatment of children and adolescents (≤18 years old) with a primary diagnosis of PTSD, as follows: (1) full PTSD, as diagnosed according to standardised diagnostic interviews, such as the Diagnostic and Statistical Manual of Mental Disorders (DSM) or International Classification of Diseases (ICD); (2) subclinical PTSD, patients who have experienced psychological trauma and report some subsequent PTSD symptoms in at least one of the four symptom clusters according to DSM-5 (re-experiencing, avoidance, hyperarousal, negative alterations in cognition and mood)15; (3) clinically significant post-traumatic stress symptoms (PTSS), defined as scoring above a validated cut-off on a rating scale.16 Trials involving patients with comorbid psychiatric disorders, such as depressive disorder or anxiety disorder, were included. Trials involving patients with acute stress disorder or adjustment disorder, combination therapies and an overall sample size of less than 10 patients were excluded. We contacted the authors to supplement incomplete reports of the original papers or provide data for unpublished studies. No restriction was applied for language. Different types and delivery formats of psychotherapies may have different effects, thus we decided a priori to consider them as independent nodes in the network meta-analysis, as applicable.17 The control conditions included no treatment (NT), treatment as usual (TAU) and waitlist (WL) (for detailed descriptions of these psychotherapies and psychological control conditions, see online supplemental appendix 2). During psychotherapies, the patients and the therapists cannot be blinded to treatment allocation.18 As a consequence, we included only trials in which patients assessed symptoms by self-rating scales as well as trials in which observer/raters were blinded.
Supplemental material
Two researchers (YX and YZ) independently screened eligible trials, extracted the relevant information and assessed risk of bias with the Cochrane Collaboration’s risk of bias V.2.0 tool.19 We resolved any discrepancies by consensus and arbitration by a panel of other investigators within the review team (XZ and PX). We also assessed the confidence of evidence contributing to each network estimate using the Confidence In Network Meta-Analysis (CINeMA) software (https://cinema.ispm.unibe.ch/).20
Outcomes
The primary outcomes were efficacy (the endpoint score from PTSD symptom scales) at post-treatment and follow-up (up to 12 months) and acceptability (all-cause discontinuation measured by the proportion of patients who withdrew from the study for any reason at post-treatment). Secondary outcomes were depressive symptoms (the endpoint score on depressive symptom scales) and anxiety symptoms (the endpoint score on anxiety symptom scales). Where PTSD symptoms were measured in a trial using more than one scale, we followed the hierarchy based on psychometric properties and appropriateness for use with children and adolescents, as published in our protocol.17 We preferred self-rated outcome over the parent-rated or clinician-rated outcome, because the effect sizes have been shown to be more conservative in the self-rated outcomes.21
Data analysis
We first performed a series of pairwise meta-analysis of direct evidence and then a network meta-analysis combining direct and indirect evidence in a random-effects frequentist hierarchical model. Details of the applied statistical approaches are provided in online supplemental appendix 3. We used standardised mean differences (SMDs, Cohen’s d) to summarise data of continuous outcomes and ORs for dichotomous outcomes, with 95% CIs, respectively.22 WL was used as the reference control condition in all forest plots.23
To assess transitivity, we compared the distribution of clinical and methodological variables across treatment comparisons. Those variables included publication year, mean age, the percentage of female patients, sample size and number of treatment session. We used the magnitude of the heterogeneity variance parameter (τ2 and total I² statistic) to assess the entire network heterogeneity across the various treatment comparisons. Incoherence between direct and indirect sources of evidence was assessed using a global (design-by-treatment inconsistency model) and a local (by calculation of the difference between direct and indirect estimates in all closed loops in the network) method.24 We also used the node-splitting method to separate evidence on a particular comparison into direct and indirect evidence to calculate the incoherence of the model.25 We used P-scores to rank interventions on the basis of the degree of efficacy or acceptability, which is based on a frequentist analogue of ‘Surface under the Cumulative Ranking Curve’.26 To determine whether the results were affected by study characteristics, we did a meta-regression for each outcome according to the following variables: publication year, mean age, the percentage of female patients, sample size, number of treatment sessions, treatment duration, follow-up duration, mean baseline severity of PTSD, risk of bias, trauma types, diagnosis criteria, source of outcome measure and psychiatric comorbidities.27 Additionally, we carried out prespecified sensitivity analyses for each outcome by omitting trials with unpublished data assessment and trials with high risk of bias. We also plotted a comparison-adjusted funnel plot and used Egger’s test to detect the presence of any dominant publication bias.28 The protocol has been registered with PROSPERO (CRD42016051786) and subsequently published.17 The minor changes to the original protocol are listed in the online supplemental appendix 4.
Findings
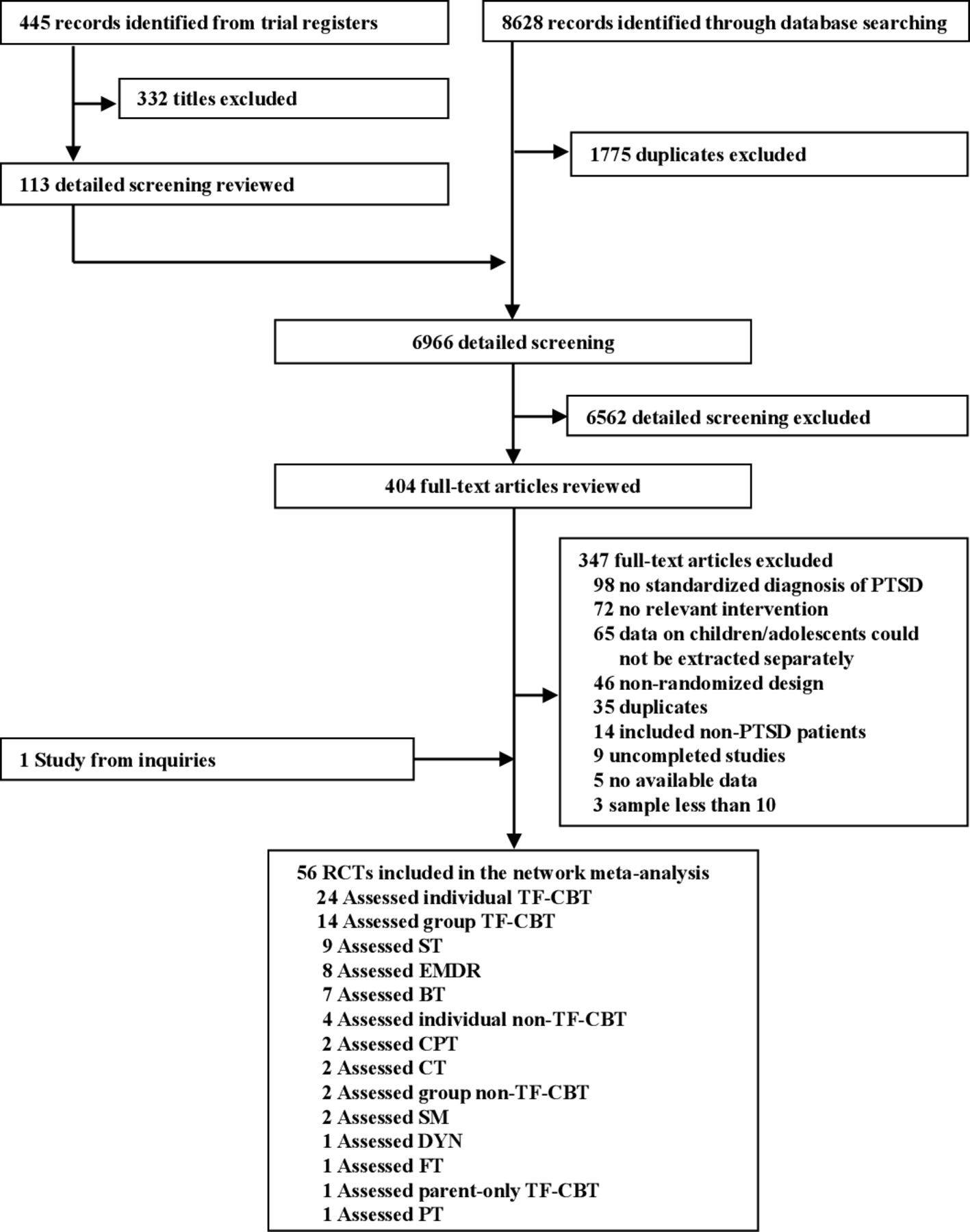
We identified 9073 citations, retrieved the full text of 404 potentially eligible articles and included 56 RCTs (5327 patients) published between 1996 and 2020 (figure 1). We retrieved unpublished information for four (7.1%) studies, and identified two (3.6%) completely unpublished trials. Overall, 14 structured psychotherapies, including group TF-CBT, individual TF-CBT, group non-TF-CBT, individual non-TF-CBT, parent-only TF-CBT, EMDR, BT, cognitive processing therapy (CPT), cognitive therapy (CT), psychodynamic therapy (DYN), play therapy (PT), stress management (SM), family therapy (FT), supportive therapy (ST) and three control conditions (WL, NT, TAU) were analysed in this study.
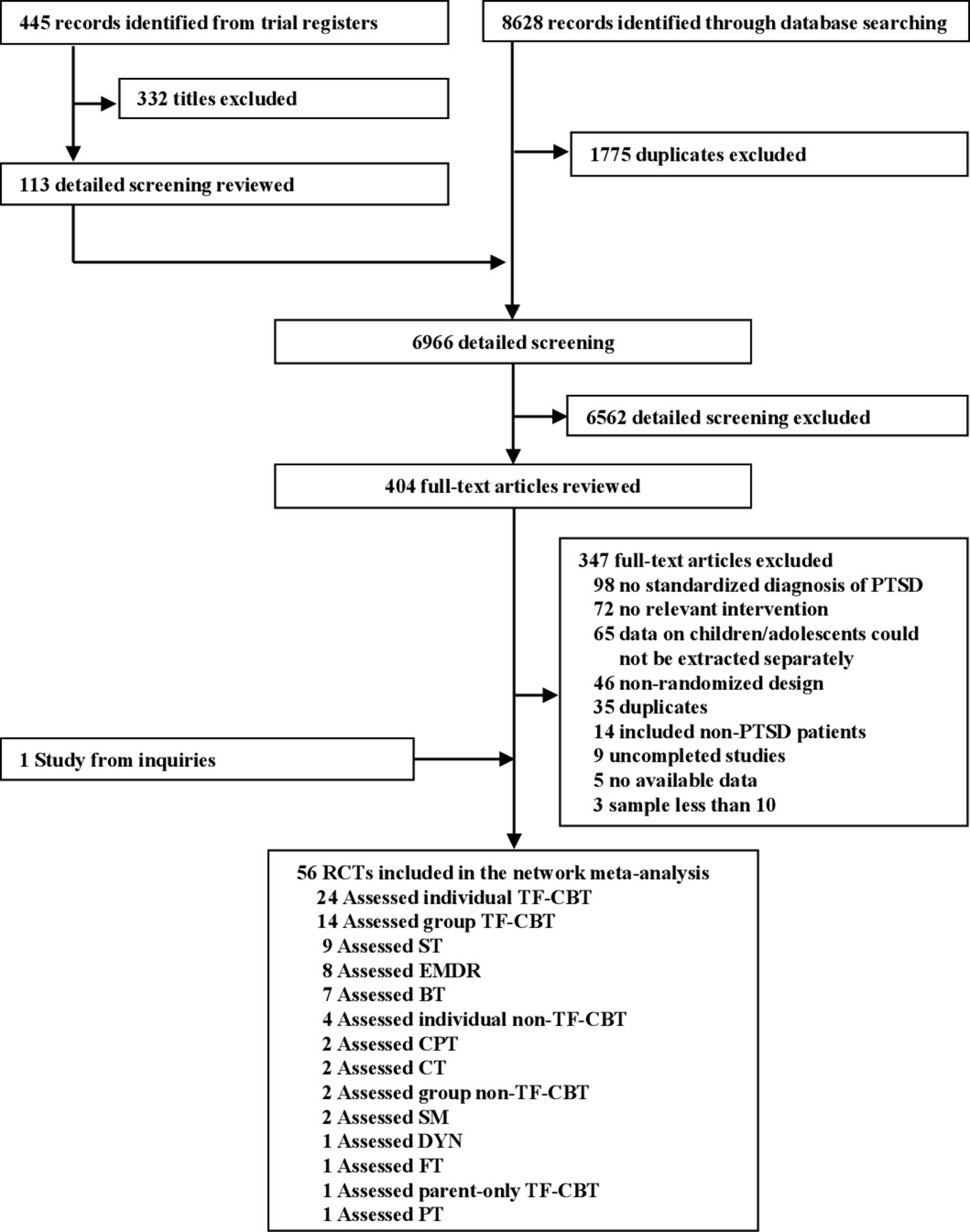
Flow chart of study selection. Some studies assessed more than one type of psychotherapy. BT, behavioural therapy; CPT, cognitive processing therapy; CT, cognitive therapy; DYN, psychodynamic therapy; EMDR, eye movement desensitisation and reprocessing; FT, family therapy; PT, play therapy; PTSD, post-traumatic stress disorder; RCT, randomised controlled trial; SM, stress management; ST, supportive therapy; TF-CBT, trauma-focused cognitive–behavioural therapy.
The characteristics of included trials are summarised in online supplemental appendices 4 and 5. The mean study sample size was 95 (range, 16–640). The mean age was 12.0 years (range, 3–18). Nineteen (33.9%) trials enrolled only children (≤12); 16 (28.6%) trials enrolled only adolescents (≥13 and ≤18); and the remaining studies enrolled both children and adolescents. More than half (56.7%) of the patients were female. Overall, 3629 (68.1%) of 5327 patients had moderate to severe PTSD, with a mean transformed baseline severity score on the Child Posttraumatic Symptom Scale of 26.1 (SD 4.5). The median duration of the treatment was 10 weeks (IQR, 7–12) and the median follow-up assessment was 6 months (IQR, 3–12) after the end of treatment. The median number of sessions was 10 (IQR, 7–12). Twenty-two (39.3%) studies were carried out in North America, 14 (25.0%) in Europe, 12 (21.4%) in Asia, 4 (7.1%) in Australia and 4 (7.1%) in Africa. Twenty-six (46.4%) studies recruited single traumatised patients, and 30 (53.6%) recruited multiple traumatised patients. Seventeen (30.3%) studies included patients with full PTSD, 6 (10.7%) with subclinical PTSD, 21 (37.5%) with PTSS and the remaining of 12 (21.4%) with mixed levels of PTSD.
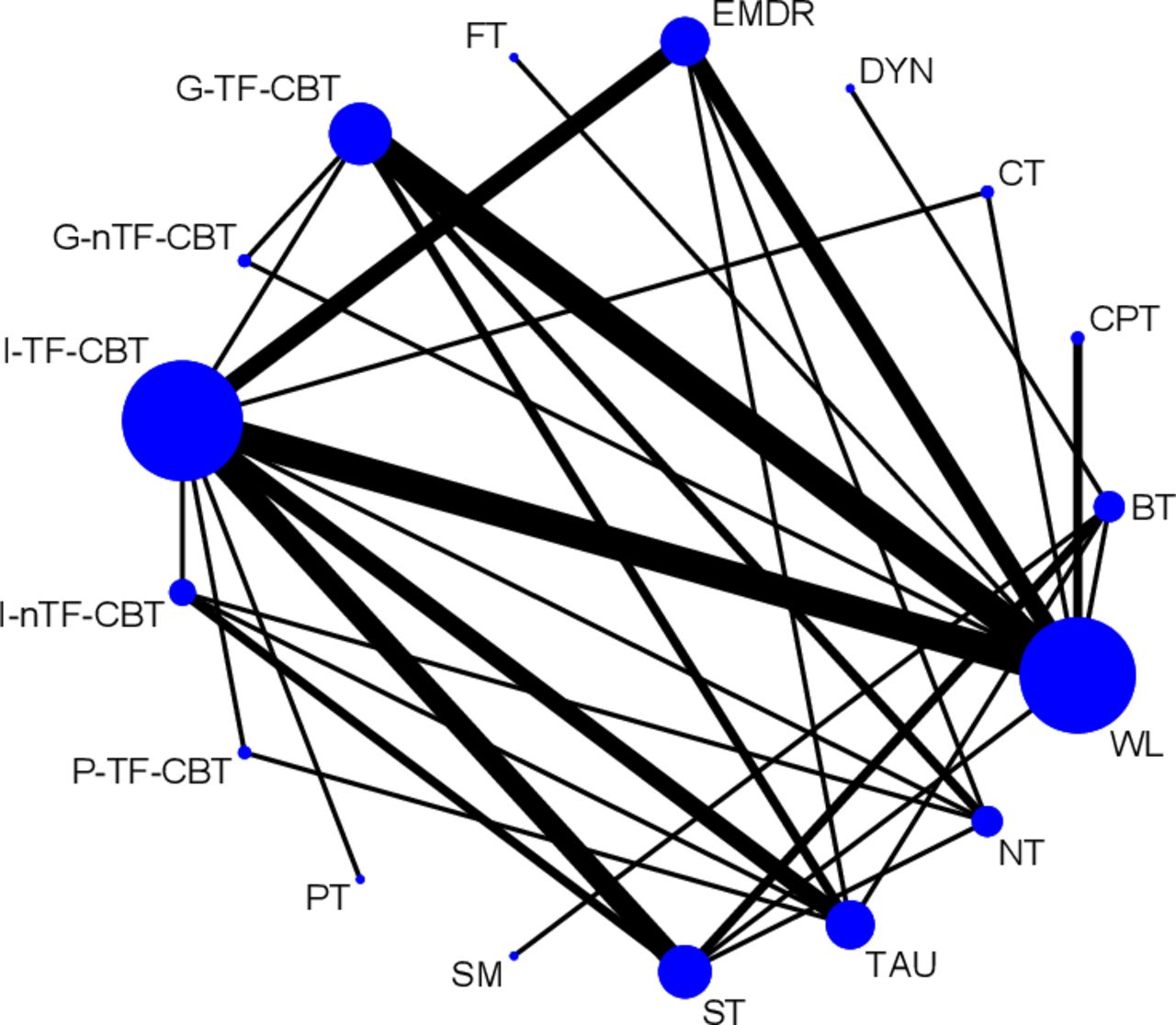
In terms of study quality, 13 (23.2%) trials were rated as high risk of bias, 26 (46.4%) trials as some concerns, 16 (28.6%) as low and 1 (1.8%) unpublished trial was impossible to assess (online supplemental appendix 6). figure 2 shows the network of eligible comparisons for efficacy at post-treatment. All psychotherapies, except for DYN, PT and SM, had at least one controlled trial, and 12 psychotherapies were directly compared with another active psychotherapy. Networks for other outcomes are displayed in online supplemental appendix 7.
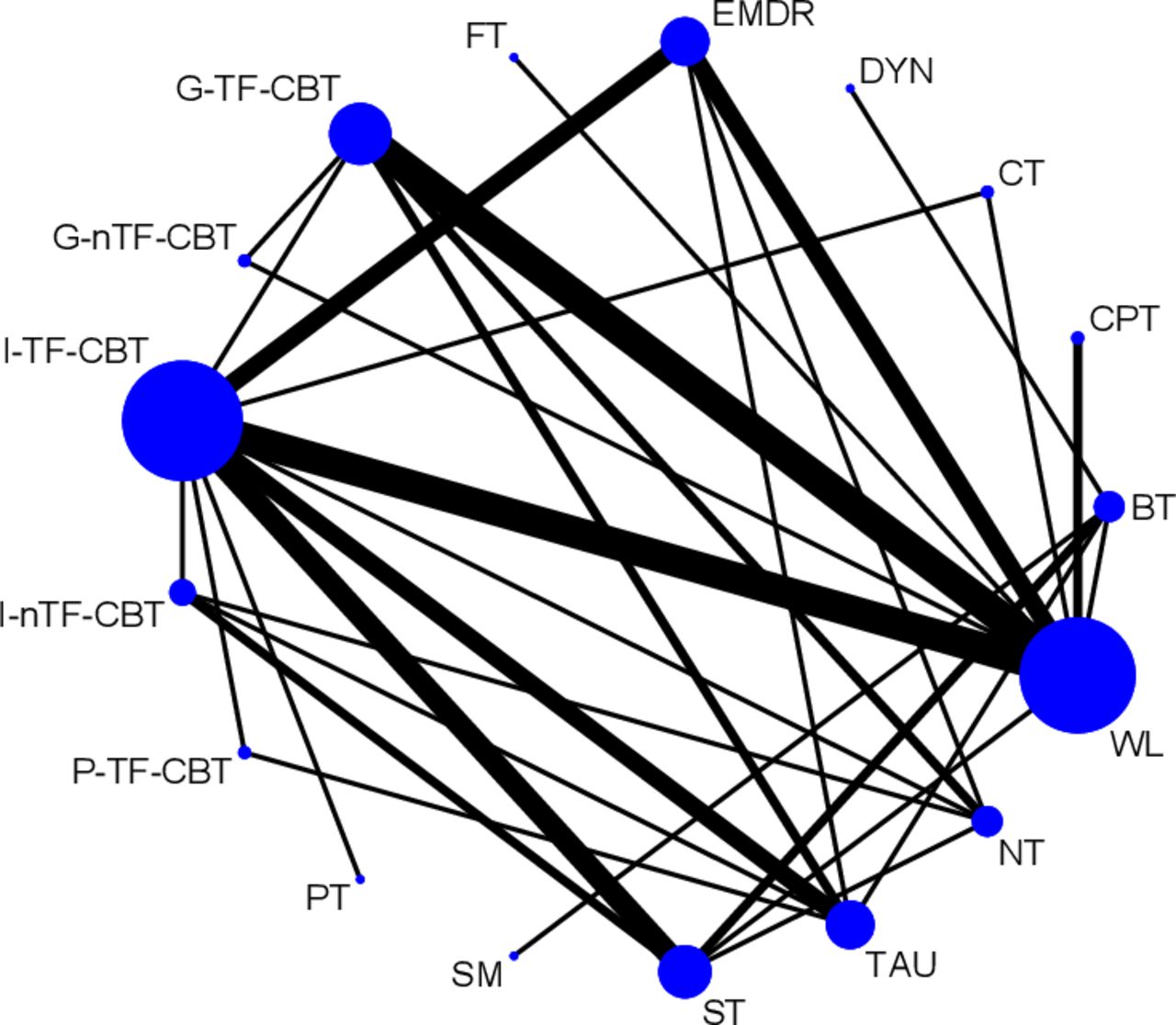
Network of eligible comparisons for efficacy at post-treatment. The width of the lines is proportional to the number of trials comparing every pair of treatments, and the size of every node is proportional to the number of randomised patients. BT, behavioural therapy; CPT, cognitive processing therapy; CT, cognitive therapy; DYN, psychodynamic therapy; EMDR, eye movement desensitisation and reprocessing; FT, family therapy; G-nTF-CBT, group non-trauma-focused cognitive–behavioural therapy; G-TF-CBT, group trauma-focused cognitive–behavioural therapy; I-nTF-CBT, individual non-trauma-focused cognitive–behavioural therapy; I-TF-CBT, individual trauma-focused cognitive–behavioural therapy; NT, no treatment; PT, play therapy; P-TF-CBT, parent-only trauma-focused cognitive–behavioural therapy; SM, stress management; ST, supportive therapy; TAU, treatment as usual; WL, waitlist.
Pairwise meta-analyses
For efficacy at post-treatment, CPT, CT, group non-TF-CBT, individual TF-CBT, ST, EMDR and group TF-CBT were more efficacious than WL. For efficacy at follow-up, CPT, BT, individual TF-CBT and group TF-CBT were more efficacious than WL. For acceptability, EMDR, individual TF-CBT and FT were associated with more dropouts than one of the control conditions; ST was more acceptable than WL. Detailed results of the other pairwise meta-analyses are shown in online supplemental appendix 8.
Network meta-analysis
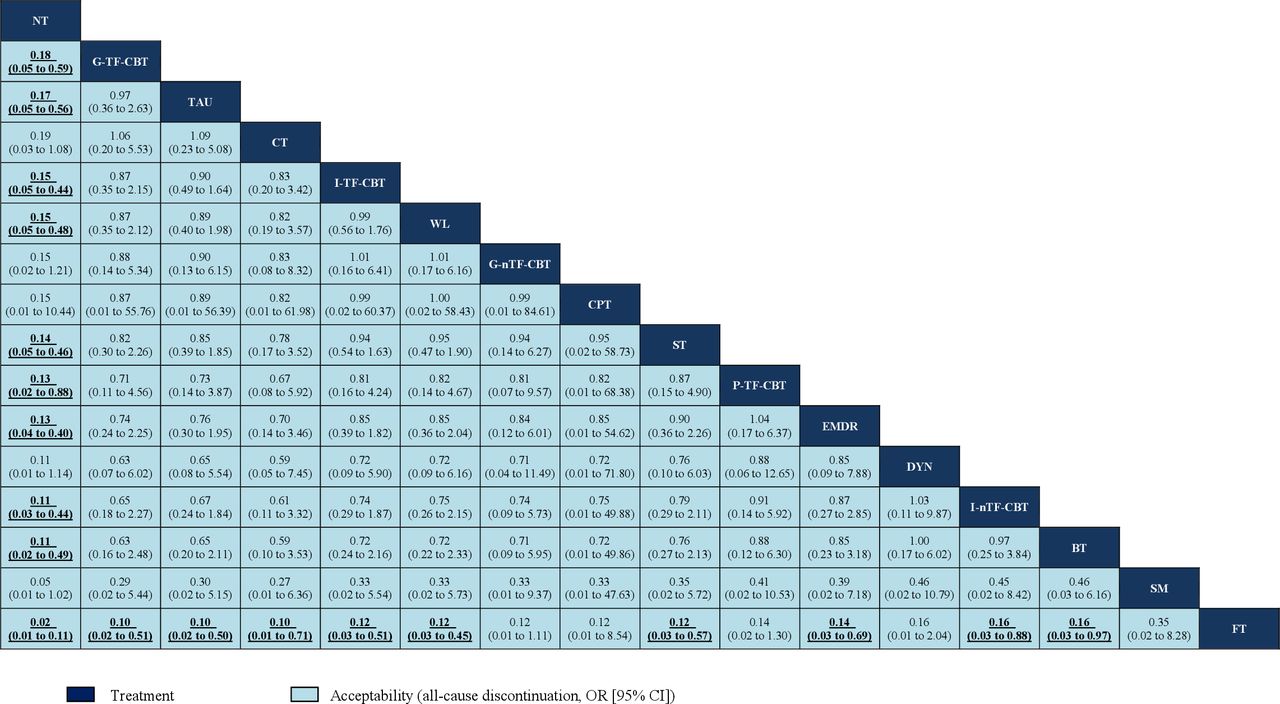
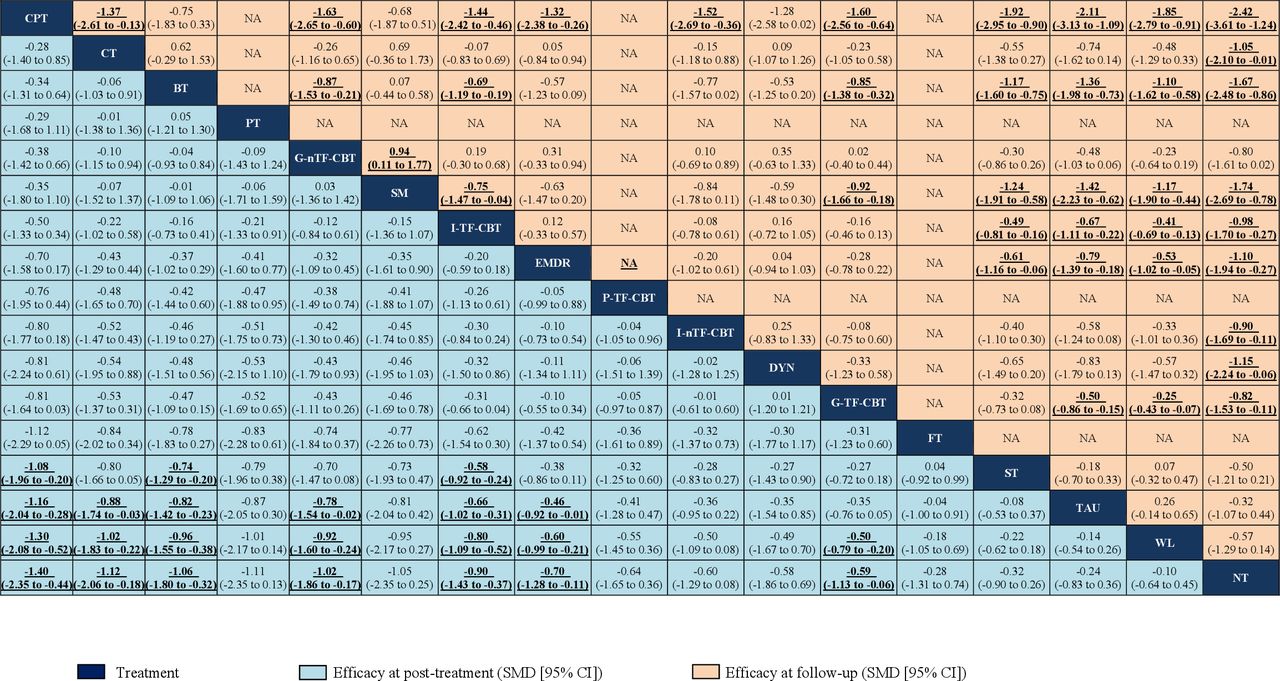
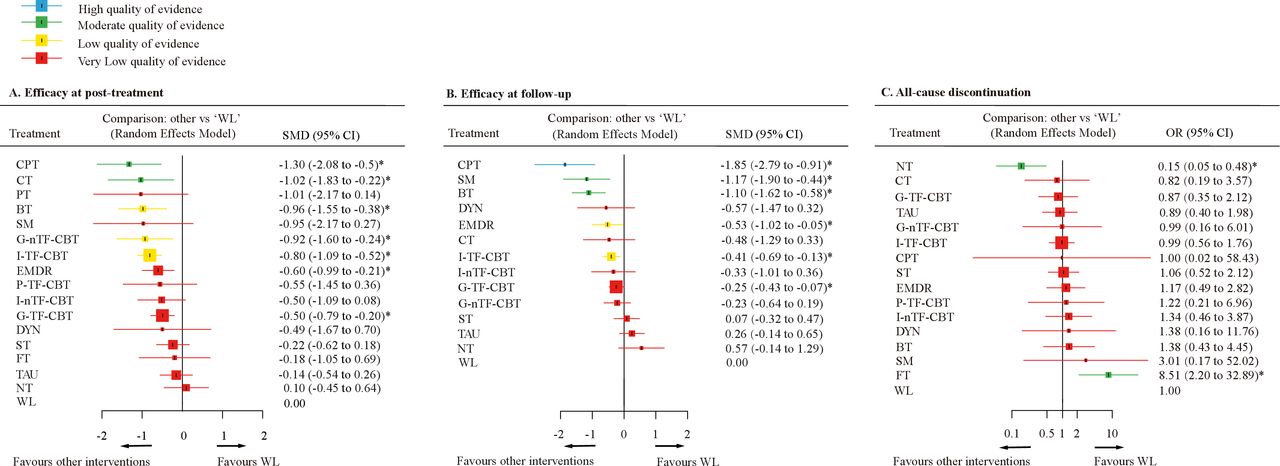
In terms of efficacy at post-treatment (54 RCTs, 4625 patients), CPT, CT, BT, group non-TF-CBT, individual TF-CBT and EMDR were significantly more effective than all control conditions (SMD range, −1.40 to −0.46). In addition, CPT, BT and individual TF-CBT were significantly more beneficial than ST (SMD range, −1.08 to −0.58, figures 3 and 4A). For efficacy at follow-up (31 RCTs, 2791 patients), CPT, BT, SM, individual TF-CBT and EMDR were more effective than all control conditions and ST (SMD range, −2.42 to −0.41), and group TF-CBT more than control conditions (SMD range, −0.82 to −0.25). Moreover, CPT, BT and SM were superior to group non-TF-CBT, individual TF-CBT and group TF-CBT (SMD range, −1.63 to −0.69, figures 3 and 4B). In terms of acceptability (50 RCTs, 4640 patients), FT was linked to more dropouts than most of psychotherapies and all control conditions (OR range, 0.02–0.16, figures 4C and 5). On the contrary, no treatment condition had fewer dropouts than most of psychotherapies, as well as TAU and WL (OR range, 0.02–0.18). Results for secondary outcomes of depressive symptoms and anxiety symptoms were not materially different from, and lent support to the findings for primary outcomes (online supplemental appendices 9 and 10).
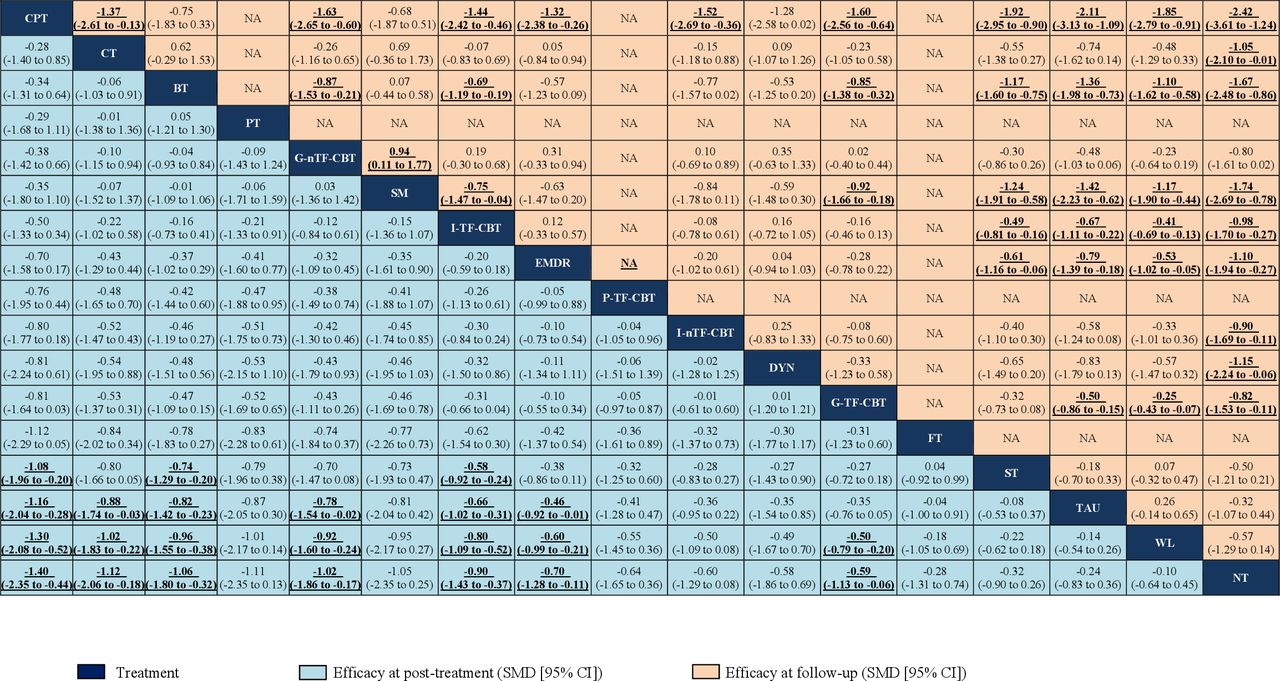
League table for efficacy at post-treatment and follow-up associated with different treatments. Treatments are ranked according to their P-scores of surface under the curve cumulative ranking for sedation starting with the best of efficacy at post-treatment. Results of the efficacy at post-treatment network meta-analysis are presented in the left lower half and results from efficacy at follow-up in the upper right half, if available. Comparisons between treatments should be read from left to right and the estimate is in the cell in common between the column-defining treatment and the row-defining treatment. For interpretation, a number less than zero favours the column-defining treatment of a cell, that is, this treatment leads to a decrease in endpoint score for PTSD symptom severity rating scales. Values depicted are standardised mean differences (SMDs) with associated 95% CIs. Significant results are in bold and underlined. BT, behavioural therapy; CPT, cognitive processing therapy; CT, cognitive therapy; DYN, psychodynamic therapy; EMDR, eye movement desensitisation and reprocessing; FT, family therapy; G-nTF-CBT, group non-trauma-focused cognitive–behavioural therapy; G-TF-CBT, group trauma-focused cognitive–behavioural therapy; I-nTF-CBT, individual non-trauma-focused cognitive–behavioural therapy; I-TF-CBT, individual trauma-focused cognitive–behavioural therapy; NA, not available; NT, no treatment; PT, play therapy; P-TF-CBT, parent-only trauma-focused cognitive–behavioural therapy; PTSD, post-traumatic stress disorder; SM, stress management; ST, supportive therapy; TAU, treatment as usual; WL, waitlist.
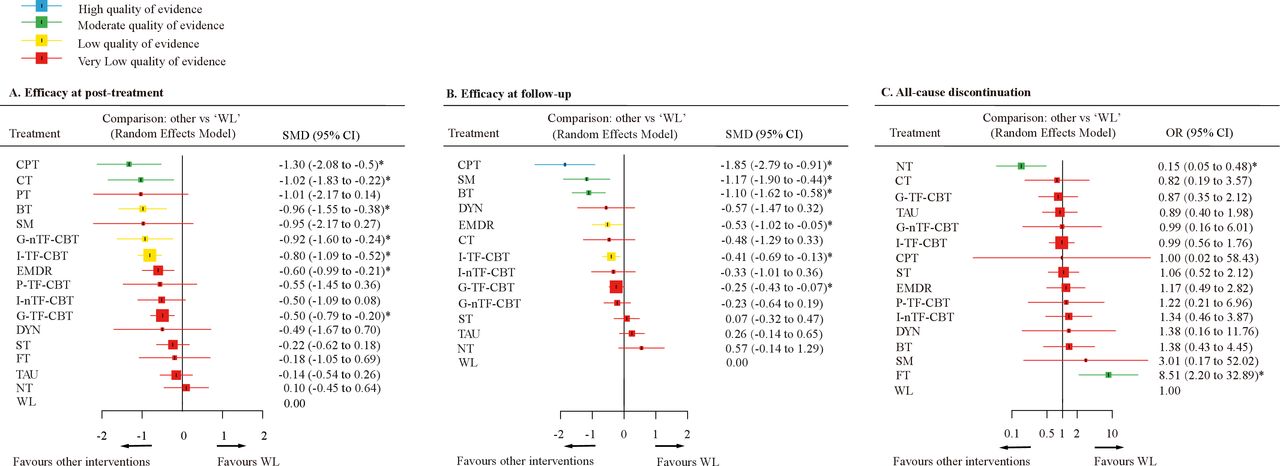
Forest plots of network meta-analysis of all trials for efficacy and acceptability. (A) Efficacy at post-treatment. (B) Efficacy at follow-up. (C) All-cause discontinuation. Interventions were compared with waitlist (WL), which was the reference compound. *Significant results. Colours indicate the confidence in the evidence for a given comparison: blue is high, green is moderate, yellow is low and red is very low. Confidence of outcomes was graded using the Confidence In Network Meta-Analysis application. BT, behavioural therapy; CPT, cognitive processing therapy; CT, cognitive therapy; DYN, psychodynamic therapy; EMDR, eye movement desensitisation and reprocessing; FT, family therapy; G-nTF-CBT, group non-trauma-focused cognitive–behavioural therapy; G-TF-CBT, group trauma-focused cognitive–behavioural therapy; I-nTF-CBT, individual non-trauma-focused cognitive–behavioural therapy; I-TF-CBT, individual trauma-focused cognitive–behavioural therapy; NT, no treatment; PT, play therapy; P-TF-CBT, parent-only trauma-focused cognitive–behavioural therapy; SM, stress management; SMD, standard mean difference; ST, supportive therapy; TAU, treatment as usual.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
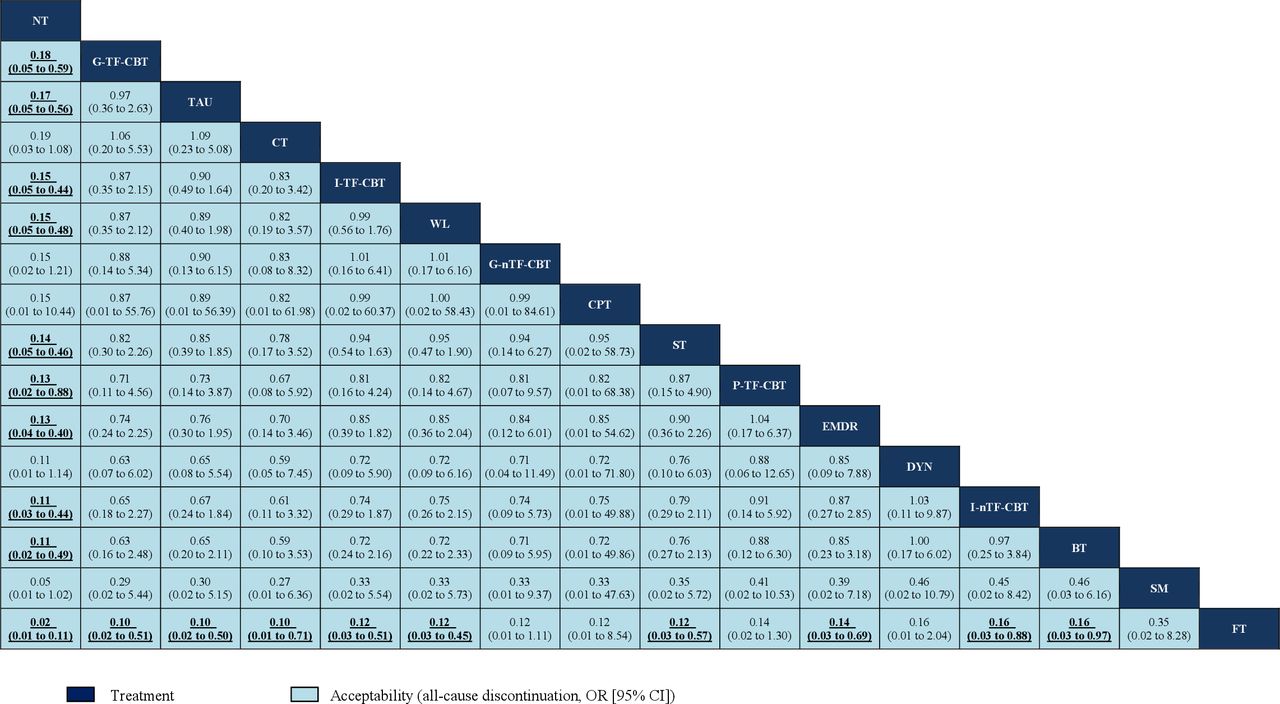
League table for all-cause discontinuation associated with different treatments. Treatments are ranked according to their P-scores of surface under the curve cumulative ranking for sedation starting with the best of acceptability. Comparisons between treatments should be read from left to right and the estimate is in the cell in common between the column-defining treatment and the row-defining treatment. For interpretation, a number less than one favours the column-defining treatment of a cell, that is, this treatment leads to a decrease in all-cause discontinuation. Values depicted are OR with associated 95% CIs. Significant results are in bold and underlined. BT, behavioural therapy; CPT, cognitive processing therapy; CT, cognitive therapy; DYN, psychodynamic therapy; EMDR, eye movement desensitisation and reprocessing; FT, family therapy; G-nTF-CBT, group non-trauma-focused cognitive–behavioural therapy; G-TF-CBT, group trauma-focused cognitive–behavioural therapy; I-nTF-CBT, individual non-trauma-focused cognitive–behavioural therapy; I-TF-CBT, individual trauma-focused cognitive–behavioural therapy; NT, no treatment; P-TF-CBT, parent-only trauma-focused cognitive–behavioural therapy; SM, stress management; ST, supportive therapy; TAU, treatment as usual; WL, waitlist.
Heterogeneity, transitivity, inconsistency and meta-regression analyses
The global I2 values were 74.6% for efficacy at post-treatment, 33.6% for efficacy at follow-up and 24.8% for acceptability (online supplemental appendix 11). The test of global inconsistency did not show a significant difference between the consistency and inconsistency models for efficacy at post-treatment (p=0.938), efficacy at follow-up (p=0.906) and acceptability (p=0.616, online supplemental appendix 11). Tests of local inconsistency showed small percentages of inconsistent loops for primary outcomes within the empirically expected range (4 of 28 loops for the efficacy at post-treatment, 0 of 6 for efficacy at follow-up and 0 of 28 for acceptability). The test of inconsistency from the node-splitting model showed significant differences between some comparisons in efficacy at post-treatment (1 of 27), efficacy at follow-up (0 of 17) and acceptability (1 of 27). The assessment of transitivity showed some of the comparisons had variable publication year, mean age, percentage of women, sample size and number of treatment sessions, for instance, one comparison involving individual TF-CBT versus ST had relatively large sample size with 229 (online supplemental appendix 12). Egger’s tests for the comparison-adjusted funnel plot did not suggest potential publication bias or small-study effect for efficacy at post-treatment (p=0.054), efficacy at follow-up (p=0.749) or acceptability (p=0.449) (online supplemental appendix 13).
Network metaregression analyses showed most modifiers (online supplemental appendix 14) did not significantly affect the efficacy and acceptability of interventions; however, we found that studies with higher risk of bias were associated with smaller treatment effects at follow-up. The sensitivity analyses did not substantially change the relative treatment effects (online supplemental appendix 14). The online supplemental appendix 15 presents the ranking of treatments based on the P-scores, which rank psychotherapies and control conditions on a continuous 0–1 scale. The contribution plot (online dataset available at http://dx.doi.org/10.17632/278y88n8r7.1) shows the percentage of contributions of each outcome from the direct comparisons for the mixed and indirect estimates. According to CINeMA evaluation, for efficacy at post-treatment, 2.2% of all comparisons were rated as moderate confidence of evidence, 7.4% as low and 90.4% as very low. For efficacy at follow-up, 3.3% of all comparisons were rated as high confidence of evidence, 25.3% as moderate, 16.5% as low and 54.9% as very low. In terms of the acceptability, 11.7% were rated as moderate confidence of evidence, 2.5% as low and 85.8% as very low (online supplemental appendix 16).
Discussion
To our knowledge, this is the most comprehensive network meta-analysis assessing psychotherapy for PTSD in children and adolescents. It is based on 56 trials including 5327 patients randomly assigned to 14 different structured psychotherapies and 3 control conditions. We extended and improved a previous study29 by searching additional unpublished databases and several international trial registers, by investigating three additional important outcomes (namely acceptability, depression symptoms and anxiety symptoms), and by using CINeMA to assess the certainty of evidence, and meta-regression analyses to explore potential sources of heterogeneity.
Effect sizes suggest that about half of the psychotherapies reduced more PTSD symptoms than control conditions, ranging between −1.40 and −0.46. Only CPT, BT and individual TF-CBT were significantly more efficacious than supportive therapy for the efficacy outcomes at post-treatment and follow-up; and CPT was among the most efficacious psychotherapies in this study. The main goal of CPT is to identify and modify dysfunctional thoughts through few formal exposure elements, Socratic dialogue and the systematic worksheets.30 In previous guidelines for PTSD in adults, CPT is one of the most extensively studied psychotherapies and has been recommended as the first-line psychological treatment,31 while it has rarely been studied with only two WL-controlled studies32 33 in adolescents. The positive treatment effect in the present study might be explained by the capability to grasp cognitive components of psychotherapies and compliance of adolescent participants.34 This evidence may not be relevant to younger children and further studies are needed to properly assess CPT in children groups.
In our analyses, TF-CBT delivered in an individual format did not result in significantly different outcomes compared with group format. However, we found that individual TF-CBT, but not group TF-CBT, was more effective than TAU and ST. Similarly, previous studies suggested that, in adults with PTSD, individual psychotherapies were associated with substantially greater effect sizes compared with group psychotherapies.35 One possible explanation is that, with an individual treatment format, the therapist can tailor psychotherapy to better meet the needs of the client than in a group-based intervention format. Other possible explanations are that because group TF-CBT for children was always conducted in classroom, it was difficult for the children to share their experiences and feelings openly in the presence of peers, or difficult to relax or concentrate during the sessions due to the school’s loud, chaotic environment.36
In our study, TF-CBT was significantly more effective than control conditions and some other psychotherapies in terms of PTSD symptoms at post-treatment and at follow-up, while non-TF-CBT did not show significant benefit compared with other psychotherapies. TF-CBT may result in less anxiety and fear for children by activating, disconfirming and confronting fear structures, and enhancing a broad spectrum of affective and behavioural functioning as well as child personal safety skills.37 These findings are consistent with the adult PTSD treatment literature that has documented the greater efficacy of TF-CBT approaches.38
According to our findings, no treatment condition had fewer dropouts than most of psychotherapies, as well as TAU and WL. However, the interpretation of the result should be done with much caution, because when someone is randomised to ‘NT’, this person can still find treatment elsewhere before post-test or follow-up (either with information about services provided in the trial or without).39 In addition, family therapy had more dropouts than most psychotherapies and all control conditions. We included only one study involving FT approaches, including their mothers, fathers and adolescent siblings.40 One possible reason is that gathering multiple family members for sessions at the same time is more difficult logistically than treating one person individually. Another possibility is suggested by the analysis from the original study showing that, dropouts from family therapy had higher levels of PTSS for family members at baseline compared with those who remained, this suggests that some of the most distressed families might not have completed the study. Thus, future work should properly examine whether the parents of young patients with PTSD may have elevated levels of PTSS or depressive and anxiety symptoms.
Our analysis has several limitations. First, in this study, the certainty of evidence for most outcomes was rated as low or very low. Although the global test of inconsistency was not significant for efficacy at post-treatment, the heterogeneity was considerable. Therefore, the interpretation and application of the results of this study should be done with caution. Second, the classification of psychotherapy for PTSD in children and adolescents remains controversial; for example, the forms and elements of CBT could be mixed, especially for some modified CBT, some studies viewed CPT as one type of CBT and combined them as one node in the network,23 29 and TAU may be very different in various mental healthcare contexts. However, the assessment of transitivity in our analysis showed most of the comparisons had similar distribution of clinical and methodological variables. Third, although we excluded trials where psychotherapy was used as a combination strategy, some patients may have taken other treatments (eg, selective serotonin reuptake inhibitors), which might have led to a variation in effects of treatment.41 Furthermore, we did not exclude trials involving patients with comorbid psychiatric disorders, because a substantial proportion of the comorbid patients with depression and anxiety are seen in real world.42 However, this may increase the risk of violating transitivity required of the network meta-analysis. Fourth, we were not able to assess some outcomes, such as adverse events discontinuation, suicidality, quality of life and functional improvement, because no available data were reported in the original studies. Fifth, even if the Egger’s test showed no significant publication bias for all outcomes, we found some potential asymmetry of funnel plots in this network meta-analysis, especially for the efficacy at post-treatment. In this study, we did our best to retrieve all available unpublished information and contacted study authors for supplementary information, but we cannot rule out the possibility that some unpublished studies are still missing.43 Finally, some findings of this study are limited by the small number and generally small size of identified studies, for example, some interventions (eg, DYN, FT, PT, parent-only TF-BT) were based on only a single study, some interventions (eg, CPT, BT) included almost adolescents but very few children and subgroup analyses or meta-regressions failed to perform for some characteristic (eg, study-conducted countries). Some meta-regression analyses (eg, mean age, mean baseline severity of PTSD, trauma types) were performed, however, they failed to show significant results, therefore, there was no enough evidence to conclude that children and adolescents with which particular characteristic could benefit more from psychological therapies than others. These data should be analysed and contextualised at the individual patient level, without access to individual patient-level data; we cannot be completely confident about the accuracy of information contained in published studies or clinical study reports.44
Conclusions
This network meta-analysis suggests that CPT, BT and individual TF-CBT appear to be good choices of psychotherapy for PTSD in young patients, while CPT appeared to produce more robust effects in adolescents. Other types of psychotherapies and different ways of delivering psychological treatment (eg, EMDR, group TF-CBT) can be alternative options. Nevertheless, there were few differences in terms of efficacy and acceptability between those psychotherapies. Future guidelines for PTSD in children and adolescents should consider this updated comparative evidence. In real-world practice, interventions need to move beyond a ‘one size fits all’ to individualising treatment, as part of this process, clinicians should consider the importance of each outcome and the patients’ preferences.
Data availability statement
Data are available in a public, open access repository. With the publication of this article, the full dataset will be freely available online in Mendeley Data, a secure online repository for research data, which allows archiving of any file type and assigns a permanent and unique digital object identifier (DOI) so that the files can be easily referenced (DOI: 10.17632/278y88n8r7.1).
Ethics statements
Patient consent for publication
Acknowledgments
Rita Rosner and Eline Rimane, Department of Psychology, Catholic University Eichstätt-Ingolstadt, Eichstätt, Germany; Elisa Pfeiffer, Clinic for Child and Adolescent Psychiatry/Psychotherapy, Ulm University, Ulm; Wietse A. Tol, Department of Public Health, University of Copenhagen, Denmark; Tim Dalgleish, Medical Research Council Cognition and Brain Sciences Unit, University of Cambridge, Cambridge, England provided unpublished data or checked the unclear data in this review. None of these persons was compensated for this work.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @And_Cipriani
Contributors XZ and PX are co-last authors. XZ and PX had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Concept and design—XZ, YZ, JRW, PC, JB, CDG, DC, DG, TT and PX. Acquisition, analysis or interpretation of data—YX, AC, JRW, PC, YZ, JB, DC, DG, AVR, TT, XZ and PX. Drafting of the manuscript—YX, XZ, JRW, PC and PX. Critical revision of the manuscript for important intellectual content—YX, AC, YZ, CDG, JRW, PC, JB, DC, DG, AVR, XZ and PX. Statistical analysis—YX, YZ, TT, CDG, XL, LF, XL, YJ, KD, AC and PX. Obtained funding—PX and XZ. Administrative, technical or material support—XZ, CDG and PX. Supervision—XZ, CDG, AC and PX.
Funding This study was supported by grant 2017YFA0505700 from the National Key Research and Development Program of China (PX); grant 2019PT320002 from the Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences (PX); grant 81820108015 from the National Natural Science Foundation of China (PX); grant 81873800 from the National Natural Science Foundation of China (XZ); grant T04040016 from the High-level Talents Special Support Plan of Chongqing (XZ); grant cstc2020jcyj-jqX0024 from the institutional funds from the Chongqing Science and Technology Commission (XZ). AC is supported by the National Institute for Health Research (NIHR) Oxford Cognitive Health Clinical Research Facility, by an NIHR Research Professorship (grant RP-2017-08-ST2-006), by the NIHR Oxford and Thames Valley Applied Research Collaboration and by the NIHR Oxford Health Biomedical Research Centre (grant BRC-1215-20005).
Disclaimer The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. The views expressed are those of the authors and not necessarily those of the National Key Research and Development Program of China, Non-profit Central Research Institute Fund of Chinese Academy of Medical Sciences, or National Natural Science Foundation of China.
Competing interests AC has received research and consultancy fees from INCiPiT (Italian Network for Paediatric Trials), CARIPLO Foundation and Angelini Pharma. JRW reported support from unrelated grants from the National Institute of Mental Health and the Institute of Education Sciences, US Department of Education; he also receives royalties for books and honoraria for various invited presentations. PC reported support for unrelated grants from the European Commission, and ZonMw, for being Chair of the Mental Health Priority Area of the Wellcome Trust in London, UK; and he receives royalties for books, and for occasional workshops and invited addresses. DC reported past consultation for or the receipt of honoraria from Otsuka, Shire, Lundbeck, Roche, Janssen and Biocodex. XZ reported receiving lecture fees from Janssen Pharmaceutica and Lundbeck. PX reported receiving lecture fees from Eli Lilly and Company, Janssen Pharmaceutica, Lundbeck and Pfizer. No other disclosures were reported.
Provenance and peer review Not commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.