Article Text

Abstract
Question Randomised controlled trials assessing treatments for anxiety, obsessive-compulsive and stress-related disorders often present high placebo response rates in placebo groups. Understanding the placebo response is essential in accurately estimating the benefits of pharmacological agents; nevertheless, no studies have evaluated the placebo response across these disorders using a lifespan approach.
Study selection and analysis We searched MEDLINE, PsycINFO, Embase, Cochrane, websites of regulatory agencies and international registers from inception to 9 September 2022. The primary outcome was the aggregate measure of internalising symptoms of participants in the placebo arms of randomised controlled trials designed to assess the efficacy of selective serotonin reuptake inhibitors (SSRIs) and serotonin and norepinephrine reuptake inhibitors (SNRIs) in individuals diagnosed with anxiety, obsessive-compulsive or stress-related disorders. The secondary outcomes were placebo response and remission rates. Data were analysed through a three-level meta-analysis.
Findings We analysed 366 outcome measures from 135 studies (n=12 583). We found a large overall placebo response (standardised mean difference (SMD)=−1.11, 95% CI −1.22 to −1.00). The average response and remission rates in placebo groups were 37% and 24%, respectively. Larger placebo response was associated with a diagnosis of generalised anxiety disorder and post-traumatic stress disorder, when compared with panic, social anxiety and obsessive-compulsive disorder (SMD range, 0.40–0.49), and with absence of a placebo lead-in period (SMD=0.44, 95% CI 0.10 to 0.78). No significant differences were found in placebo response across age groups. We found substantial heterogeneity and moderate risk of bias.
Conclusions Placebo response is substantial in SSRI and SNRI trials for anxiety, obsessive-compulsive and stress-related disorders. Clinicians and researchers should accurately interpret the benefits of pharmacological agents in contrast to placebo response.
PROSPERO registration number CRD42017069090.
- anxiety disorders
- adult psychiatry
- child & adolescent psychiatry
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Trials assessing treatments for anxiety, obsessive-compulsive and stress-related disorders report high placebo response rates.
No studies have evaluated the placebo response associated with selective serotonin reuptake inhibitors (SSRIs) and serotonin and norepinephrine reuptake inhibitors (SNRIs) during acute treatment of individuals diagnosed with anxiety, obsessive-compulsive and stress-related disorders using a lifespan approach.
WHAT THIS STUDY ADDS
We found a large placebo response associated with SSRIs and SNRIs and this estimate was moderated by patient diagnosis and presence of a placebo lead-in period.
No significant differences across age groups were found concerning placebo response.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The placebo response in anxiety spectrum disorders is likely to be moderated by intrinsic factors of psychopathology and factors associated with study design.
This knowledge may lead to the development of better clinical trials in the field and may also add information for clinicians when interpreting the benefits associated with SSRIs and SNRIs.
Background
Placebo response estimates in randomised controlled trials (RCTs) designed to assess the efficacy of medications for treatment of anxiety, obsessive-compulsive and stress disorders are robust, with response rates in placebo groups reaching rates of almost 40%.1 2 Understanding the central aspects of placebo response, such as the magnitude and the moderators of the effect size, is important to maximise researchers’ ability to detect true pharmacological benefits.3 4 This knowledge may lead to the development of better clinical trials in the field, possibly by reducing the costs of developing new drugs, and ultimately by accelerating clinical availability of drugs for this population. It may also provide information to clinicians for the interpretation of the benefits of pharmacological agents, which should be seen in contrast to placebo response, adding insight into how people diagnosed with these mental health conditions improve their symptoms. Furthermore, clinical care could be improved by facilitating shared decision making for medication use, allowing a discussion of precise estimates of the true pharmacological benefits in specific symptom domains, considering individual patients’ preferences and social constraints.
In comparison with the vast literature on psychosis5 6 and depression,2 7 systematic reviews on anxiety, obsessive-compulsive and stress disorders are scarce. Available evidence shows that placebo response varies significantly between different types of anxiety disorders in adults.1 8 9 One study in adults has shown that placebo response is significantly higher in trials designed to assess panic disorder (PD) when compared with trials concerning social anxiety disorder (SAD) and generalised anxiety disorder (GAD)1; other studies expanding the investigation to obsessive-compulsive disorder (OCD) showed a lower placebo response in trials involving this disorder if compared with anxiety disorders and post-traumatic stress disorder (PTSD).9 10
Another issue never explored in child anxiety literature is the extent to which placebo response varies across developmental phases. The perceived placebo response differs between adults and children for several different disorders.11 Although a recent study indicated that children and adolescents diagnosed with depression present smaller placebo response and smaller medication effect when compared with adults,12 previous evidence suggests that the lower efficacy of medications among paediatric patients may be explained by the higher placebo response, rather than the lower response to the active agent itself.13 14 This might also be the case for anxiety disorders, which are often comorbid with depression.15 16 Differences in placebo response due to distinct diagnostic categories were also observed in children. One study showed that patients diagnosed with SAD exhibited lower placebo response rates,8 while others found that children with OCD responded less to placebo than children with anxiety disorders or depression.17 18
Beyond diagnosis and age, aspects that have been reported to moderate the placebo response in anxiety disorders are related to (a) study design factors, such as number of study sites, recruitment setting, sample size and frequency of follow-up visits; (b) patient-related factors, such as expectancy and baseline illness severity; and (c) publication-related factors, such as year of publication and funding.1 8 9 17 18 However, most studies fail to adjust for moderators altogether, which might be a preferable approach given the effects of moderators might be additive or overlapping between studies.
The current literature is limited in important ways. First, no studies have contrasted the placebo response in internalising symptoms across anxiety, obsessive-compulsive and stress disorders using a lifespan approach. Therefore, little is known about the comparative placebo response between children and adults with emotional disorders. Second, previous meta-analyses did not include unpublished trials, which might bias the average estimates for placebo responses. Third, these studies did not allow the inclusion of multiple outcome measures of the same study and were often restricted to specific assessment instruments, perhaps leading to biased estimates and limited statistical power. Finally, previous reviews1 8 9 17 18 included no more than half of the trials we identified here and may have missed important findings due to limited statistical power. Therefore, an update is warranted.
Objective
We conducted a systematic review and meta-analysis to estimate the magnitude of placebo response in internalising symptoms in RCTs of selective serotonin reuptake inhibitors (SSRIs) or serotonin and norepinephrine reuptake inhibitors (SNRIs) for anxiety, obsessive-compulsive or stress-related disorders over the lifespan and to explore potential moderators.
Study selection and analysis
This study is part of a three-level network meta-analysis designed to evaluate the efficacy of SSRIs, SNRIs and placebo in internalising symptoms of children and adults diagnosed with anxiety, obsessive-compulsive or stress-related disorders.19 This review is registered in PROSPERO (registration number CRD42017069090) and is reported as recommended by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (online supplemental S1 table A).20
Supplemental material
Search
For this meta-analysis, we included RCTs assessing the efficacy of SSRIs, SNRIs and placebo in subjects with a primary diagnosis of any anxiety disorder, OCD or stress-related disorder according to standard operationalised diagnostic criteria (Feighner criteria, any International Classification of Diseases (ICD) version, Diagnostic and Statistical Manual of Mental Disorders-III (DSM-III), Diagnostic and Statistical Manual of Mental Disorders-III-Revised (DSM-III-R), Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV), Diagnostic and Statistical Manual of Mental Disorders-IV-Text Revision (DSM-IV-TR) and Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5). Studies could compare any SSRI or SNRI with each other (ie, head-to-head studies), with the same medication using distinct doses (ie, different dose studies) or with a placebo group; nevertheless, all RCTs had to include a placebo arm. Trials with any kind of previous intervention (eg, medication after psychotherapy period) or selection based on treatment resistance were excluded. No restriction was used regarding comorbidities with any other mental disorder (eg, depression, bipolar disorder), participants’ age and sex, blindness of participants and researchers, date of publication, and study language.
We searched MEDLINE, PsycINFO, Embase and Cochrane using keywords related to study design, interventions and assessed disorders, from inception to 23 April 2015 and updated on 9 September 2022 (search strings are depicted in online supplemental S1 text A). Electronic database searches were supplemented with manual searches for published and unpublished RCTs registered in ClinicalTrials.gov, ISRCTN registry, European Clinical Trials Database, Pan African Clinical Trials Registry, International Federation of Pharmaceutical Manufacturers & Associations, Australian New Zealand Clinical Trials Registry, Food and Drug Administration database and pharmaceutical companies’ databases. The reference lists of the included RCTs and relevant reviews were inspected, and experts were asked to indicate additional trials.
Data extraction, quality assessment and outcome variables
Four reviewers (MdAC, MdBJ, LSM and JF), all psychiatrists, independently reviewed the full-text articles and supplementary materials, extracting the relevant information from the included trials with a predefined data extraction sheet. A fifth reviewer (NPG) double-checked all data entries. Disagreements and inconsistencies were resolved by consensus of all review group members. For companion papers, we included the most informative and complete study report. Any outcome of interest reported in only one of these studies was also extracted within the same trial data.
We defined the primary outcome as the aggregate measure of internalising symptoms, which encompasses several domains of emotional distress. This included domains comprising anxiety (generalised anxiety, social anxiety, somatic, panic, specific phobias, separation anxiety), obsessive-compulsive, post-traumatic and stress symptoms, as well as overall symptom severity. All baseline data and outcome measures reported between 6 and 26 weeks of follow-up were included in the analysis. We considered outcomes as close to 12 weeks as possible. If information at 12 weeks was unavailable, we preferred the timepoint closer to 12 weeks; if equidistant, the longer. The secondary outcomes were response and remission rates as defined by the investigators in the original studies (online supplemental S1 table B).
Risk of bias appraisal was performed using the Cochrane risk of bias tool version 1.21 We classified studies as having low risk of bias if none of the domains in the instrument was rated as high risk of bias and three or less were rated as unclear risk; moderate if one was rated as high risk of bias or none was rated as high risk of bias, but four or more were rated as unclear risk; and all other cases were rated as having high risk of bias.22 We assessed small study effects through a funnel plot.
Statistical analysis
The meta-analysis of the primary outcome and the meta-regression analysis were conducted using three-level models with two random variables: study and assessment instrument. This method considers similarities within studies when retrieving distinct outcome measures from the same study and between studies when retrieving outcomes with the same scale.23 In these models, the placebo response was estimated by standardised mean differences (SMD) from baseline to endpoint mean scores of any internalising symptom assessed in placebo intervention groups, assuming a correlation between initial and final means of 0.25, as indicated by previous evidence.24 When not available, the SDs of baseline means were imputed using the mean of reported SDs of outcome measures evaluated with the same assessment instrument.25 We estimated the effect sizes for the aggregate estimate of internalising symptoms and for specific symptom domains through stratified analysis by age groups, as defined in the primary studies. Meta-analysis for response and remission rates was done using random-effect models. We estimated the between-study variance through τ2 estimates and heterogeneity through I 2.
The multiple meta-regression model considered the following variables: diagnosis, sample age (categorised a priori as ‘children/adolescents’ and ‘adults/elderly’), sampling, concomitant benzodiazepine use, placebo lead-in period, time to outcome measure, data analysis method, publication year, baseline severity of symptoms, number of sites, sample size at baseline, number of drug arms, number of visits and study funding source. We classified study funding as academic, governmental or non-profit, industry, or unclear according to the funding sources statement of the primary studies. We categorised all studies that did not explicitly report academic, governmental or non-profit, or industry funding sources or did not present any funding source statement as having an unclear funding. We also conducted meta-regression analyses stratified by age groups, as reported by the primary studies, considering all clinical and methodological moderators with sufficient data for convergence of the meta-regression models. Pairwise comparisons of significant moderators in the multiple meta-regression model were assessed as post-hoc analyses to explore the meaning of the moderation effects. Tests of moderators for diagnoses in the multiple regression model were performed using Wald-type χ2 test. We also investigated whether placebo–drug differences could be affected by placebo response differently depending on the diagnostic group. We tested if the SMD in the placebo group affected placebo–drug differences differently as a function of the main diagnostic category in the multiple meta-regression model of our previous study, which investigated placebo–drug differences for all SSRIs and SNRIs.19 We assessed the informant effect through subgroup analyses of clinician ratings and self-rating scores of specific symptom domains in each included diagnosis.
Corresponding 95% CIs for all measures were estimated. Two-sided p values less than 0.05 were considered statistically significant. All analyses depict sample size (n), number of studies (k) and number of outcome measures (o). Analyses were performed using R (V.3.5.1) with ‘metafor’ package.26
Findings
Description of the included studies
These data are part of a previously published meta-analysis.19 A total of 5655 titles and abstracts were screened, and 420 full-text articles were evaluated for inclusion (online supplemental S1 figure A). We included 122 published trials and 13 unpublished reports (135 studies), which reported 366 outcome measures, comprising 12 583 participants. Of these, we included 95 studies, which reported 263 outcome measures, comprising 9632 participants, in the meta-regression analysis. Reasons for exclusion in the meta-regression analysis were lack of information about the number of sites (23 studies), number of visits (21 studies) and publication year (13 studies), moderators in our multiple meta-regression model. A total of 107 studies reported response rates and 52 reported remission rates. The characteristics of the included studies are depicted and summarised in online supplemental S1 tables C-F.
Primary and secondary outcomes
For the primary outcome, we estimated a placebo response of −1.11 (SMD, 95% CI −1.22 to −1.00), with significant heterogeneity between studies (I 2=95.9%, p<0.001). The placebo response estimates for all included outcome measures are depicted in figure 1. We found significant SMDs, which could be classified as moderate to high, for all specific symptom domains in all specific age groups. Only GAD symptoms were evaluated in all specific age groups and was the only symptom domain assessed in RCTs specifically designed to evaluate adolescents and elderly participants (table 1).
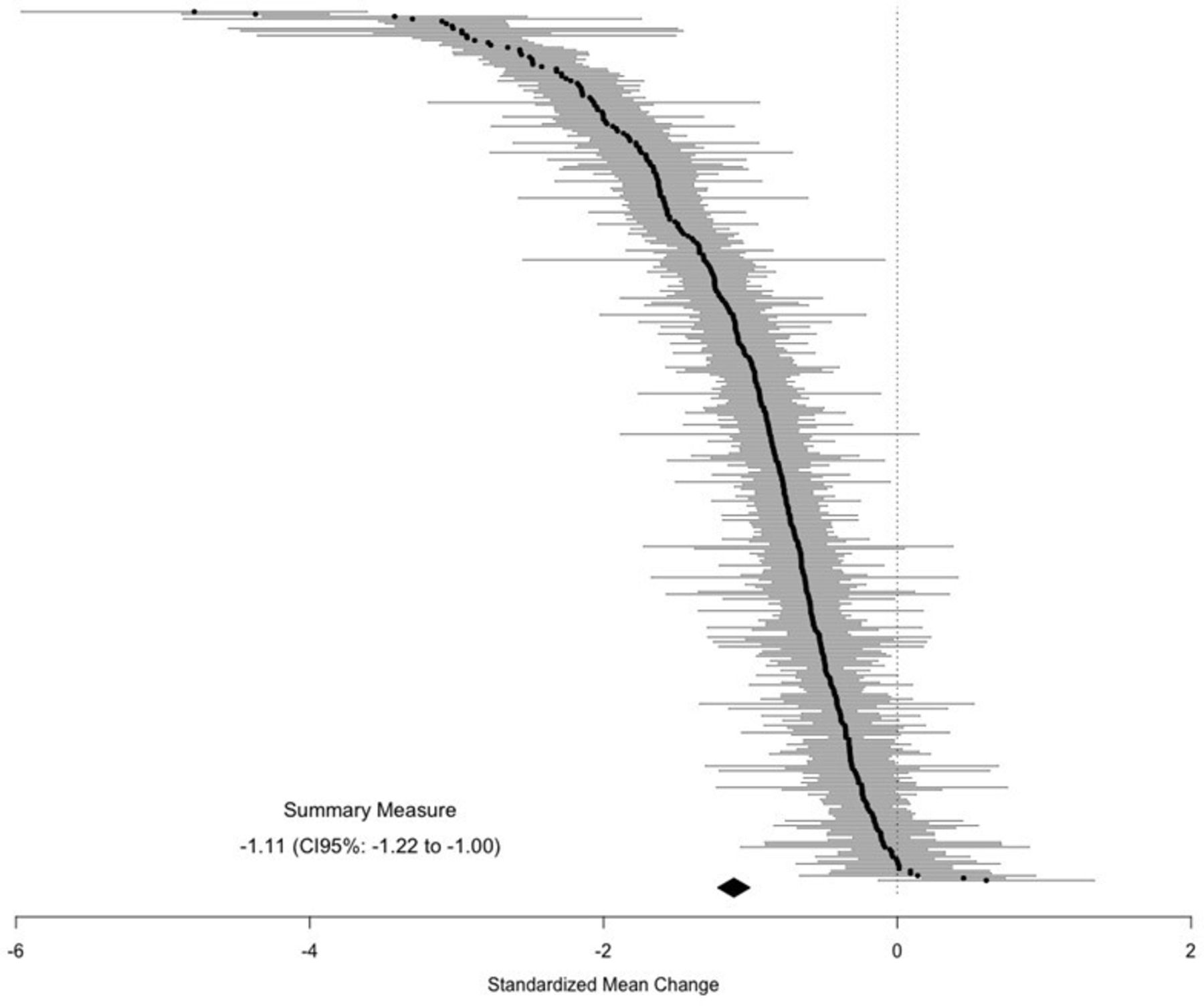
Summary measure of placebo response’s standardised mean difference.
Placebo response for each symptom domain by age group
We estimated a response rate of 37.4% (95% CI 34.8 to 40.1, p<0.001, I 2=89.5%, k=107). The results were very similar when restricting to trials using intention-to-treat (ITT) (37.3%; 95% CI 34.5 to 40, p<0.001, I 2=89.5%, k=94) and for trials using the score of 1 or 2 (‘Very much improved’ or ‘Much Improved’) in the Clinical Global Impressions - Improvement (37.3%; 95% CI 33.3 to 41.1, p<0.001, I 2=89.9%, k=50), the most commonly used criterion for defining response. The remission rate was estimated at 24% (95% CI 20.9 to 27.1, p<0.001, I 2=89.9%, k=52) and the results were very similar for trials using ITT (25%; 95% CI 21.2 to 27.9, p<0.001, I 2=90.9%, k=45).
Placebo response estimates ranged from −0.60 to −1.68 when estimated through self-report scores and from −0.68 to −1.60 when based on clinician rating scores. Subgroup analyses indicated that clinicians estimate larger improvement of GAD symptoms when compared with estimates of self-report scales (table 2).
Placebo response for each symptom domain as estimated by self-report and clinician-rated scores
Meta-regression analysis
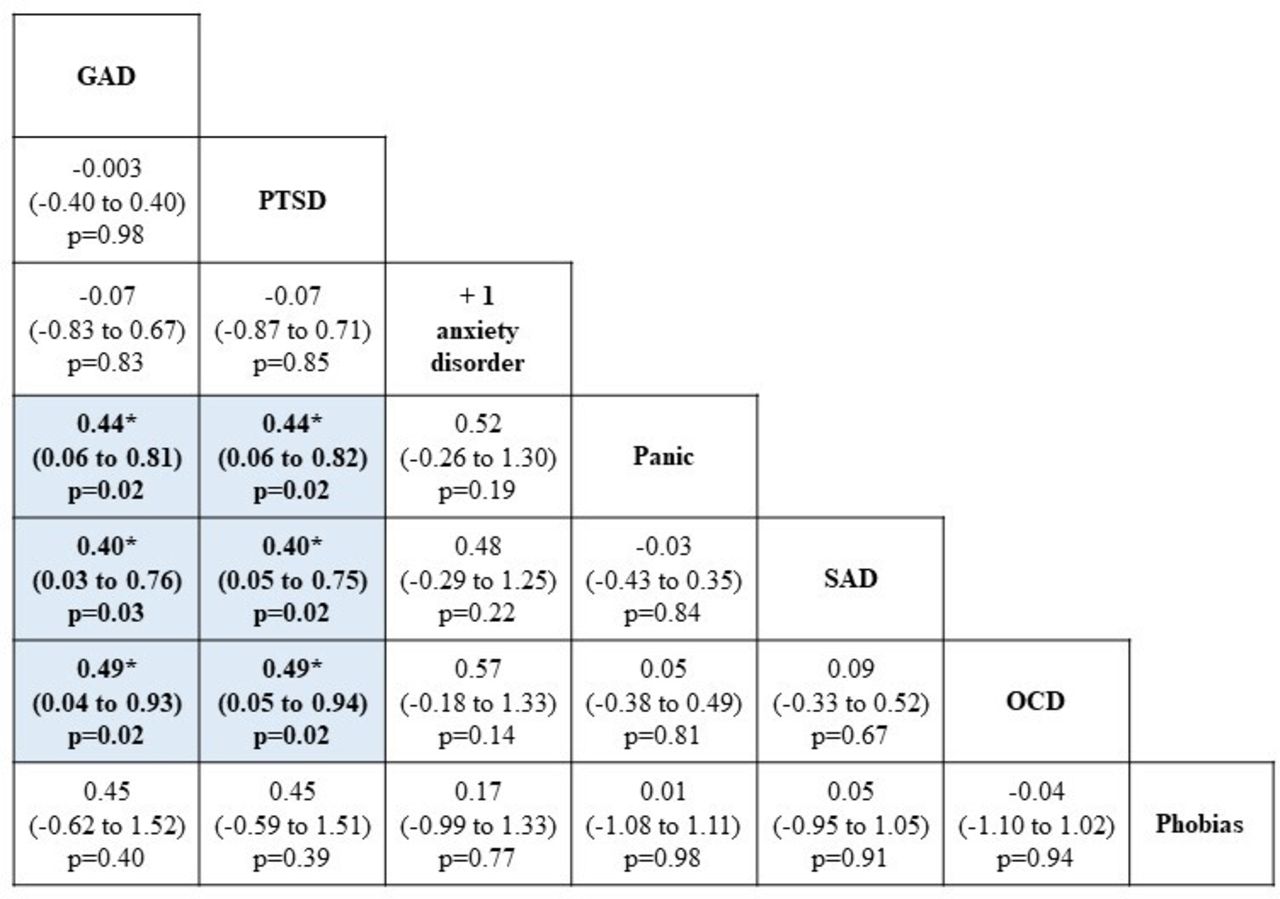
Our meta-regression analysis identified that diagnosis and placebo lead-in period moderated the placebo response after accounting for all other moderators included in the multiple meta-regression model. Pairwise comparisons revealed that participants diagnosed with GAD and PTSD had larger placebo response estimates than those diagnosed with PD, SAD and OCD (figure 2). In addition, the presence of a placebo lead-in period significantly reduced the placebo response (SMD=0.44, 95% CI 0.10 to 0.78). Age group, sampling, concomitant use of benzodiazepines, time to outcome measure, data analysis method, publication year, baseline severity of symptoms, number of sites, number of drug arms, sample size and number of visits did not moderate the placebo response. Full results of the meta-regression model can be seen in table 3. Studies that were excluded from the meta-regression analysis reported an effect size (SMD=−1.08, 95% CI −1.29 to −0.87) similar to the estimate of the primary analysis, which included all studies.
{kind=link}
{kind=link}
Pairwise comparisons of diagnosis of participants for the placebo response. Comparisons between diagnoses should be read from left to right and estimates above 0 indicate higher placebo response for the column-defining diagnosis. Effect sizes are reported as standardised mean differences. +1 anxiety disorder, more than one anxiety disorder; GAD, generalised anxiety disorder; OCD, obsessive-compulsive disorder; panic, panic disorder; PTSD, post-traumatic stress disorder; SAD, social anxiety disorder. Shaded cells and * indicate significant differences.
Multiple multilevel meta-regression model for placebo response on the aggregate measure of internalising symptoms
We also conducted meta-regression analyses stratified by age groups, considering all clinical and methodological moderators with sufficient data for convergence of the meta-regression models. We found significant moderation effects when assessing specific age groups:
Adults: participants diagnosed with GAD presented larger placebo response estimates than those diagnosed with PD (SMD=1.00, 95% CI 0.23 to 1.77) and OCD (SMD=1.20, 95% CI 0.44 to 1.96). Trials that allowed concomitant benzodiazepine use showed larger response estimates than those with unclear exclusion criteria (SMD=2.27, 95% CI 0.96 to 3.57). Head-to-head studies presented higher placebo response than different-dose trials (SMD=1.87, 95% CI 0.79 to 2.96) and placebo-controlled RCTs (SMD=2.13, 95% CI 0.89 to 3.38) (online supplemental S1 table G).
Adults/elderly: presence of a placebo lead-in period significantly reduced the placebo response (SMD=0.82, 95% CI 0.18 to 1.46). Larger sample sizes were associated with larger placebo response (SMD=−0.006, 95% CI −0.01 to −0.001) (online supplemental S1 table H).
Elderly: individuals diagnosed with more than one anxiety disorder presented larger placebo response estimates than those diagnosed with GAD (SMD=1.01, 95% CI 1.89 to 0.13). Trials with participants who presented less severe internalising symptoms at baseline were associated with larger placebo response (SMD=−0.01, 95% CI −0.02 to −0.002) (online supplemental S1 table I).
There were no significant mediation effects of clinical and methodological moderators in children/adolescent trials (online supplemental S1 table J). Only two RCTs specifically designed to evaluate adolescents were included; given so, there were no sufficient data to perform the meta-regression analysis.
Risk of bias assessment
Thirty (22.22%) trials were rated as having a high risk of bias, 67 (49.62%) trials as moderate and 38 (28.14%) as low risk of bias (online supplemental S1 table K and online supplemental S1 figure B). Visual inspection of the funnel plot suggests that small studies gave different results from larger studies (online supplemental S1 figure C).
Post-hoc analysis
We found a significant placebo mean difference by diagnostic category interaction in the multiple meta-regression model of placebo–drug differences (likelihood ratio test=18.6, p=0.002). Pairwise analysis revealed that placebo mean changes were associated with larger placebo–drug differences in the OCD group (SMD=0.478, p=0.003), panic group (SMD=0.324, p<0.001) and SAD group (SMD=0.364, p=0.006), if compared with the PTSD group. No other significant differences were found for pairwise comparisons between diagnoses.
Conclusions and clinical implications
Our results indicate a large placebo response in anxiety, obsessive-compulsive and stress-related disorders in SSRI and SNRI RCTs across the lifespan regarding symptom improvement, response and remission rates. Estimates of placebo response were moderated by patient diagnosis (larger in GAD and PTSD, if compared with PD, SAD and OCD) and use of a placebo lead-in period. In accordance with findings concerning a patient’s diagnosis, symptom domains related to GAD and PTSD were associated with larger placebo response estimates. No moderation effects were found for other variables, including age group, sampling, concomitant use of benzodiazepines, time to outcome measure, data analysis method, publication year, baseline severity of symptoms, number of sites, number of drug arms and number of visits. Subgroup analysis of specific age groups did not indicate significant differences in placebo response estimates; nevertheless, we found distinct moderators of effect for some specific age groups. Post-hoc analysis revealed that placebo response in OCD, PD and SAD leads to higher placebo–drug differences than in PTSD. Although we found that clinician-rated assessments present larger placebo response when compared with estimates based on self-report measures of GAD symptoms, there were no significant differences concerning the informant effect in other symptom domains.
Prior studies showed that placebo response estimates range from 0.65 to 1.29 in anxiety disorders,27 28 with response rates reaching 41%.1 In line with previous evidence, we found a large effect size for the placebo response, reinforcing the notion that the placebo response is very strong in anxiety disorders and possibly larger than in other conditions such as depression and psychosis. Even though we did not compare these effects directly, other meta-analyses have shown that the effect sizes for placebo response in major depression were, on average, 0.37,2 while for psychosis the effect sizes were 0.33,29 both with substantial heterogeneity. Thus, participants diagnosed with anxiety, obsessive-compulsive or stress-related disorders may be particularly prone to higher placebo response regarding internalising symptoms.
Our data contribute to cumulative evidence involving GAD and PTSD as the diagnoses with the strongest placebo responses.1 9 10 In paediatric population, there is also a tendency towards a lower response to placebo in patients diagnosed with OCD and SAD when compared with those diagnosed with other anxiety disorders.8 18 30 Our results showed that placebo response in OCD, PD and SAD leads to larger placebo–drug differences than in PTSD, which reinforces the importance of accounting for placebo response differences when comparing treatment benefits for different anxiety, obsessive and stress-related disorders.
As the efficacy of medications depends on the magnitude of the difference between the drug and the placebo, a large placebo response associated with SSRIs and SNRIs might obscure the clinical observation of the real benefits of medications for specific disorders, given clinicians are incapable of distinguishing drug and placebo responses. Although our previous findings on the efficacy of medications indicate a large variation in effect size estimates within drug arm trials for distinct SSRIs and SNRIs (SMD=−1.33 to −2.33), placebo–drug comparisons did not indicate significant differences between medications when estimating effect sizes through placebo–drug differences (SMD, −0.43 to −0.68).19 These findings should reinforce the importance of estimating the benefit of medications in meta-analyses by estimating between-group SMDs (ie, placebo–drug differences within trials), avoiding potentially misleading comparisons based on pre–post SMDs, since these estimates would not indicate which proportion of the effect size is caused by the intervention itself or by other factors, such as the placebo response.24
Regarding other moderators, placebo response appears to be moderated by placebo lead-in periods in RCTs, opposing our previous results concerning the efficacy of medications which did not indicate a significant moderation effect of placebo lead-in periods on placebo–drug differences (SMD=0.03, 95% CI −0.15 to 0.22),19 in line with previous negative findings in clinical trials for anxiety and depression and in RCTs of antidepressants.31 These results suggest that although placebo lead-in periods do not moderate estimates of the medication effect, probably due to similar distribution of placebo responders between treatment arms, it might be especially relevant to account for this moderator when estimating the placebo response.
We did not find a moderation effect for age groups and found similar placebo response estimates across all specific age groups; nevertheless, GAD was the only symptom domain assessed in all groups. In line with previous evidence,30 OCD symptoms were associated with smaller placebo response in children and adolescents, while PTSD was associated with larger placebo response in children, adolescents and adults. Moreover, we found distinct moderators of effects for specific age groups. While placebo lead-in period, concomitant benzodiazepine use, comparator, sample size and baseline severity of symptoms moderated placebo response estimates in adults and elderly, we did not identify significant moderators in RCTs designed to assess children and adolescents. This finding suggests that clinical and methodological moderators should be further explored in the paediatric population.
Comparisons between self-report and clinician-rated scores indicated that clinicians overestimate the placebo response in GAD symptoms, in accordance with findings on depression, which indicated that clinician-rated instruments resulted in larger effect sizes than those estimated by self-report measures.32 Moreover, previous evidence examining the relation between different informants in the assessment of individuals diagnosed with GAD indicated that presence of coexisting depression accounted for 17% of the variance in clinician severity ratings.33 Hence, researchers should account for the effect of comorbidity on clinician-rated scores and possibly consider including assessment instruments of both informants in RCTs designed to evaluate improvement of symptoms of GAD.
Our study has some important limitations. First, heterogeneity was high, and even though moderators explained the heterogeneity in effect size estimates there was considerable residual heterogeneity to be further explained. Second, we found evidence of small study effects; therefore, our results regarding average estimates should be interpreted cautiously. Third, the placebo response was evaluated using pre–post effect size estimates as a proxy, so these estimates may be biased by other aspects, such as repeated measure effects or the natural course of psychopathology. Fourth, some negative findings should be interpreted cautiously due to the possibility of false negative results potentially related to high variance or lack of statistical power in some meta-regression analyses. Despite these limitations, our study also has important strengths. First, to the best of our knowledge, this is the largest meta-analysis assessing the placebo response in trials with anxiety, obsessive-compulsive and stress-related disorders. Second, this is the first study on this topic to use a lifespan approach, being able to assess the role of placebo response in distinct age groups. Finally, we used a three-level design, allowing us to accommodate all outcome measures reported in each trial, preventing possibly biased estimates and increasing statistical power.19
In summary, placebo response in anxiety spectrum disorders is likely moderated by intrinsic factors of psychopathology and factors associated with study design, such as use of lead-in periods. These results may be an important step towards a better understanding of a phenomenon as complex as the placebo response in common disorders such as anxiety, obsessive-compulsive and stress-related disorders.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Acknowledgments
We thank all authors who kindly provided additional information and data regarding their studies for this meta-analysis. We thank our funding agencies, Fundo de Incentivo à Pesquisa/Hospital de Clínicas de Porto Alegre (FIPE/HCPA), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) and Child Mind Institute (CMI) for the financial support for this work.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
LSM and NPG are joint first authors.
LSM and NPG contributed equally.
Contributors LSM, NPG, MdAC, MdBJ, JF, LS and GS conceived and designed the study. LSM, MdAC, MdBJ and JF did the literature search and extracted the data. LSM and GS did the analyses and drafted the manuscript. All authors contributed to the interpretation of the findings and subsequent edits of the manuscript. LS, GGM, PC, DSP and GS provided overall supervision to the project. LSM is the guarantor.
Funding This study was financed in part by Fundo de Incentivo à Pesquisa/Hospital de Clínicas de Porto Alegre (FIPE/HCPA), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES), Finance Code 001, Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq), Brazilian federal government agencies, and Child Mind Institute (CMI). Daniel Samuel Pine was supported by NIMH Intramural Research Program Project ZIA-MH002781.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.