Article Text

Abstract
Background Suicide-related behaviours are common in young people and associated with a range of negative outcomes. There are few evidence-based interventions; however, cognitive behavioural therapy (CBT) shows promise. Internet delivery of CBT is popular, with potential to increase reach and accessibility.
Objective To test the effectiveness of an internet-based CBT program (Reframe-IT) in reducing suicide-related behaviours, depression, anxiety, hopelessness and improving problem solving and cognitive and behavioural skills in school students with suicide-related behaviours.
Methods A parallel randomised controlled trial testing the effectiveness of Reframe-IT plus treatment as usual (TAU) compared with TAU alone in reducing suicidal ideation, suicide attempts, depression, hopelessness, symptoms of anxiety, negative problem orientation and cognitive and behavioural skill acquisition was undertaken. We recruited students experiencing suicidal ideation from 18 schools in Melbourne, Australia, between August 2013 and December 2016. The intervention comprised eight modules of CBT delivered online over 10 weeks with assessments conducted at baseline, 10 weeks and 22 weeks.
Findings Only 50 of the planned 169 participants were recruited. There were larger improvements in the Reframe-IT group compared with the TAU group for the primary outcome of suicidal ideation (intervention −61.6, SD 41.6; control −47.1, SD 42.3, from baseline to 22-week follow-up intervention); however, differences were non-significant (p=0.593). There were no increases in distress in the majority of participants (91.1%) after completion of each module. Changes in depression and hopelessness partly mediated the effect of acquisition of CBT skills on suicidal ideation.
Conclusions The trial was underpowered due to difficulties recruiting participants as a result of the complex recruitment procedures that were used to ensure safety of participants. Although there were no significant differences between groups, young people were safely and generally well engaged in Reframe-IT and experienced decreases in suicidal ideation and other symptoms as well as improvements in CBT skills. The study is the first online intervention trial internationally to include young people demonstrating all levels of suicide risk.
Clinical implications Integration of internet-delivered interventions for young people with suicide-related behaviour may result in reductions in these behaviours. Further research is needed, but researchers should feel more confident about being able to safely undertake research with young people who experience these behaviours.
Trial registration number ACTRN12613000864729.
- mental health
Statistics from Altmetric.com
Background
Suicide-related behaviours, including suicide attempts and suicidal ideation, are common among young people. Up to 24% of young people aged 12–17 year have reported suicidal ideation, and 7%–11% have reported a 12-month prevalence of suicide attempts.1 These behaviours are associated with a range of negative outcomes, including suicide and other forms of premature mortality.2 3 The prevention of suicide is a priority, yet there remains a lack of high-quality intervention research for suicidal youth.4 Cognitive behavioural therapy (CBT) has been one of the most commonly investigated interventions for young people with suicide-related behaviours and has shown promise in several trials.5 6 It is also used extensively in the treatment of adolescent depression.7 Given depression is the most common risk factor for suicide-related behaviours, CBT is an obvious intervention to further investigate. Internet-based CBT has the potential to be more accessible and less stigmatising than traditional, face-to-face models of therapy,8 9 and it has been shown to be an effective and cost-effective form of treatment for depression and anxiety in adolescents.10 Although there is emerging evidence regarding the impacts of web-based and mobile suicide prevention interventions in young people,11 there is currently little published research.
Programs that are password protected, and practitioner prescribed and supported, tend to have better rates of adherence.12 13 Given this, and that school well-being staff are considered helpful by students when it comes to mental health-related difficulties,14 development of internet-based CBT program for delivery by school well-being staff would seem a logical next step. In response to this, we developed and tested a youth-specific Internet-based program for school students at risk of suicide as indicated by the presence of suicide-related behaviours. The program, called Reframe-IT, was designed to be delivered and supported by school well-being staff. In pilot testing, there was a reduction in suicidal ideation, depressive symptoms and hopelessness.15 Pilot data also showed that Reframe-IT did not induce either distress or suicidal ideation, and that participants found Reframe-IT acceptable and useful.16 The pilot study was small and uncontrolled; therefore, the program required testing in a randomised controlled trial (RCT).
Objective
The primary objective of this study was to examine whether or not participation in the Reframe-IT program resulted in reduced suicide-related behaviours (primarily suicidal ideation, but also suicide attempts). We also aimed to examine the safety of delivering the intervention and young people's engagement in the program. Additionally, we examined its impact on self-rated symptoms of depression, clinician-rated levels of depression, hopelessness, symptoms of anxiety, negative problem orientation and cognitive and behavioural skill acquisition. Finally, we also sought to understand how cognitive and behavioural skill acquisition might impact on symptom reduction.
Methods
The study was a parallel RCT testing the efficacy of Reframe-IT plus treatment as usual (TAU) against TAU alone. The trial has been registered (ACTRN12613000864729; 5 August 2013), and the protocol for the trial has been published.17 Ethics approval was obtained from the University of Melbourne Human Research and Ethics Committee (number: 1033768).
Setting
The study was conducted by Orygen, The National Centre of Excellence in Youth Mental Health, with recruitment occurring between August 2013 and December 2016. Orygen has an integrated clinical service, research and education and training platform. The study was implemented in school settings in the North West metropolitan Melbourne catchment area (the same as serviced by the clinical services of Orygen). All secondary schools in the study catchment area were invited to participate; 18 schools were recruited in a staggered manner over the duration of the study.
Participants
High school students were eligible for inclusion if they:
were aged 13 to 19 years;
were engaged with a well-being staff member;
had experienced any level of suicidal ideation within the 4 weeks; we did not exclude those with very severe levels of suicidal ideation or those who had engaged in self-harm including a suicide attempt.
Exclusion criteria included presence of intellectual disability, psychotic symptoms and/or inability to speak English. Presence of psychosis symptoms was assessed using the abbreviated version of the Comprehensive Assessment of At Risk Mental State, which only assesses for positive symptoms.18
Interventions
The Reframe-IT intervention has been described in detail in the published protocol.17 Briefly, it comprised eight modules of CBT delivered over a 10-week intervention period. Each participant had access to his or her own personalised web page accessed via secure login. The student well-being staff member administered the program at school. Once each individual module was completed in the presence of the school staff member, participants were able to access it from home, 24 hours a day. The program had no social networking function.
Standard CBT approaches7 were delivered, but there was a specific focus on suicidal thinking and behaviours. There were eight modules covering each of the following topics: engagement and problem identification, emotional recognition and distress tolerance, identification of negative automatic thinking, behavioural activation—help seeking, behavioural activation—activity scheduling (including relaxation techniques), problem solving, and cognitive restructuring, and a wrap up session. This content was delivered via a series of video diaries made by young people, with an adult ‘host’ character highlighting the CBT approaches that had been demonstrated in the context of the video diaries. There were two activities per module. The site had a message board through which the participant could communicate with a research therapist (each of whom was a registered clinical psychologist) who also checked completed activities and responded with personalised but standardised messages. Finally, it contained a series of fact sheets covering a range of related topics, including managing suicidal thoughts, plus downloadable relaxation MP3s.
Treatment as usual
TAU, which was also received by the participants allocated to Reframe-IT, consisted of contact with the school well-being staff, as well as any additional outside mental health service provision normally available such as treatment by psychologists, psychiatrists, other counsellors, general practitioner support, social work and treatment at enhanced primary care integrated youth mental health services (headspace), and medication.
Measurement and outcomes
The primary outcome of the study was reduced suicidal ideation as measured by the Suicidal Ideation Questionnaire (SIQ).19
Secondary outcomes included the following:
Suicide attempt, measured by a specifically designed questionnaire that asked the participant (1) whether they had attempted suicide since the last assessment, and, if yes, (2) how many attempts they had made.
Self-rated depressive symptoms, measured by the Reynolds Adolescent Depression Scale-2 (RADS-2).20
Clinician-rated depressive symptoms, measured by the Children's Depression Rating Scale Revised (CDRS-R).21
Self-rated hopelessness, measured by the Beck Hopelessness Scale (BHS).22
Self-rated anxiety, measured by the Multidimensional Anxiety Scale for Children (MASC).23
Problem solving, measured by the Negative Problem-Oriented Questionnaire (NPOQ).24
CBT skill acquisition, measured by the Cognitive-Behavioural Therapy Skills Questionnaire (CBTSQ).25 This measure provides an overall score of general CBT skill acquisition as well as two subscale scores, one measuring acquisition of behavioural activation skills (Cognitive-Behavioural Therapy Skills Questionnaire—Behavioural Activation; CBTSQ-BA) and one measuring acquisition of cognitive restructuring skills (Cognitive-Behavioural Therapy Skills Questionnaire—Cognitive Restructuring; CBTSQ-CR).
Website use, measured by extraction of back-end metrics of how many modules and how much of each module was completed, how many activities were completed and how often the message board was used.
Safety of delivery of the intervention, assessed by a specifically developed scale that asked young people to rate on a scale of 0 to 3 whether they had no, mild (no plan or intent), moderate (some level of intent and vague plan) or severe thoughts of suicide (clear plan with intent) immediately before they began each module and immediately after they completed the module. School welfare staff were made aware of these ratings in real time and were available to respond to participants indicating suicidal ideation after completion of a module.
The validity and the reliability of each of these measures were judged as at least adequate for all the measures used, which were also chosen in terms of their appropriateness for the age group (see protocol paper for full justification of measures).17
Assessments were conducted at baseline, 10 weeks (postintervention) and 22 weeks (12-week follow-up) at the participating schools by a trained research assistant. All self-report outcome measures with the exception of the CDRS-R were administered online. The baseline assessment information was fed back to school well-being staff and often resulted in referral for additional mental health services.
Randomisation, treatment allocation and blinding
After baseline assessment, the study coordinator (JR), who had no role in the assessment, randomised eligible participants into the treatment or control group. This was done via an online randomisation computer program set up by an independent statistician (HPY). This program used a random number generator to produce a randomisation list, which was stratified by school. The program did not allow knowledge of treatment next to be allocated before the participant details were entered into the computer. The relevant school well-being staff member was automatically notified of treatment allocation for participants via email.
Because of the nature of the intervention, it was not possible for school staff to be blind to intervention. In addition, the study coordinator (JR) and the study psychologists (SH, SR and SB) were not blinded in order to enable the website to be moderated. The research assistants (EB, GC and KT) conducting outcome assessments and the statistician conducting the analysis (HPY), however, remained blind to treatment allocation during the study.
Statistical analysis
Analysis was by original assignment groups. Descriptive statistics including frequencies, means and SD were calculated for all outcome variables. Linear mixed-effects model analysis was used to compare the intervention and control groups in terms of the change in continuous outcome measures from baseline to the two follow-up time points. For each outcome measure, school was included as a random factor to account for possible school effect. Fisher's exact test was used to compare frequency of suicide attempt cases between groups.
The association between acquisition of cognitive and behavioural skills and improvement in suicide ideation and the possible mediating effect of symptom improvement, including depression, hopelessness, anxiety and negative problem solving orientation, were examined using Pearson correlation.
Effect size and statistical power
The initial power calculation was based on changes in suicidal ideation from baseline to 10 and 22 weeks measured by the SIQ.19 A sample size of 169 was required to detect medium effect sizes based on an alpha of 0.05 and power of 0.80, accounting for intra-cluster correlation to take account of the clustering effect of the schools, and a dropout rate of 24%.
Findings
Due to difficulty in recruitment, only 50 participants were randomised: 24 to the control group and 26 to the intervention group. Between one and seven participants were recruited from each school. A 10-week follow-up was completed by 21 and 18 participants in the control and intervention groups, respectively (12.5% vs 30% dropout rate), and the 22-week assessment was completed by 17 and 13 participants in the control and intervention groups, respectively, with a corresponding dropout rate of 29.2% and 50% (figure 1).
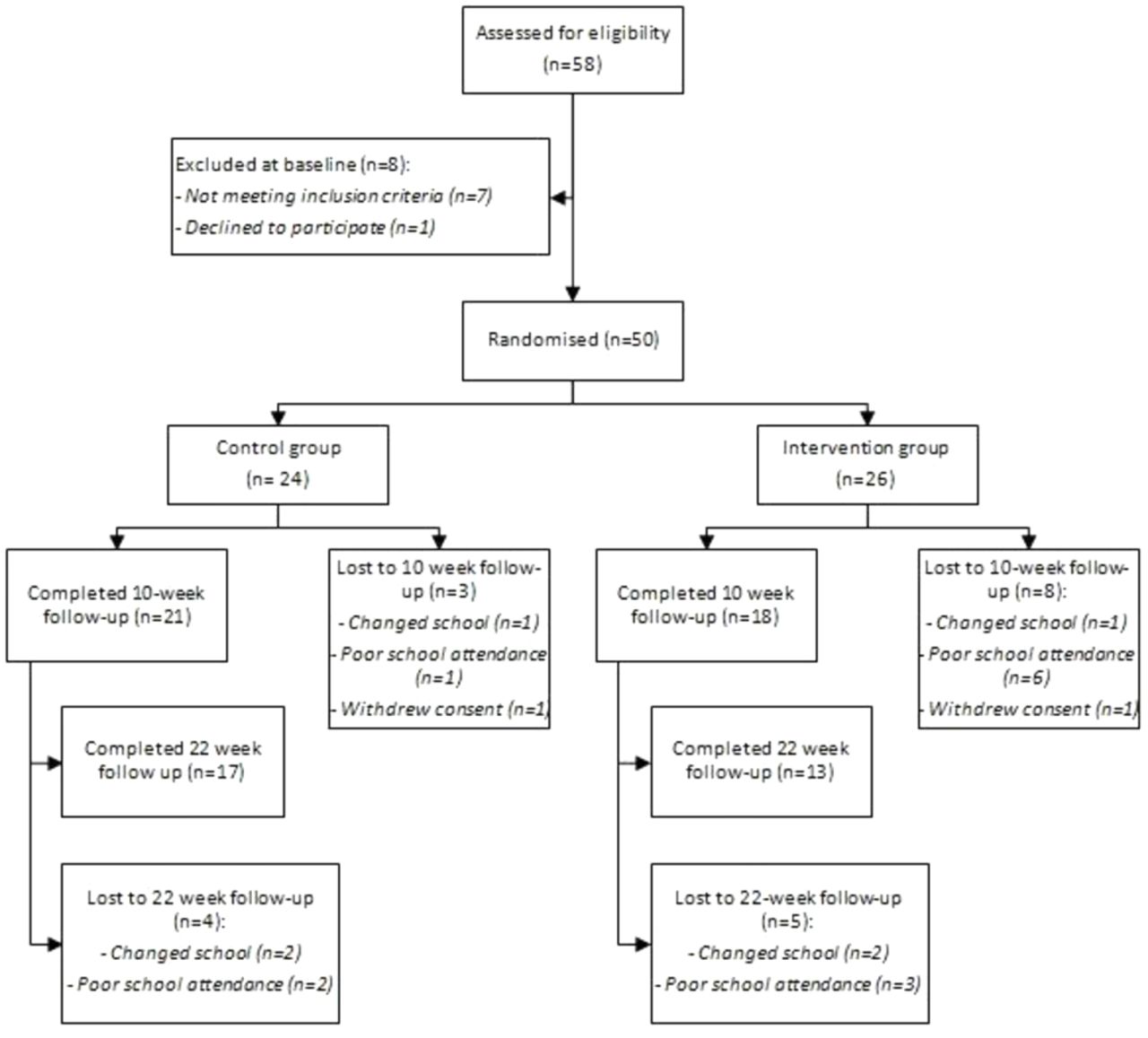
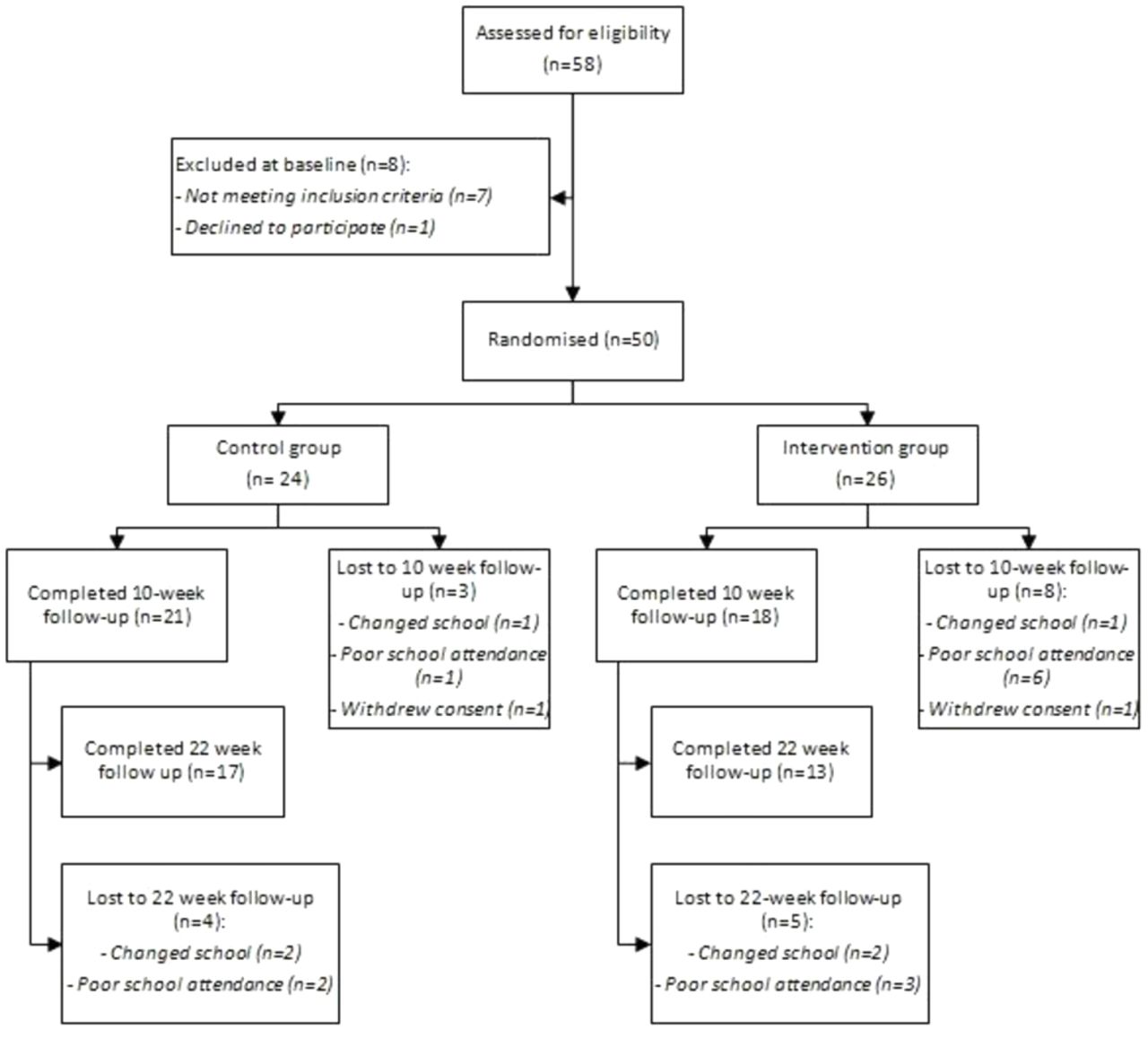{kind=link}
Consolidated Standards of Reporting Trials (CONSORT) flow diagram.
The characteristics of all randomised participants are shown in table 1. Most of the participants were female (82%), and the gender distribution between the two groups was similar. The majority of participants were in year 9 or 10 at school (year 12 is the final year at school in Australia). Of note were the elevated scores of participants at baseline across the outcome measures (see table 2). For example, both the self-report and the clinician-rated depression scores at baseline were above the suggested cut points, indicating clinically significant symptomatology. One hundred and two previous suicide attempts were reported at baseline across 12 people (one young person reported 75 suicide attempts); twice as many people in the intervention group had a history of suicide attempt than controls. A number of young people were receiving care from a mental health professional in addition to seeking support from the school counsellor.
Baseline characteristics for all randomised participants
Baseline mean and SD for each of the outcome measures and changes from baseline to 10-week follow-up and 22-week follow-up for the intervention and control groups
Intervention use
The average number of modules commenced by the 26 participants in the intervention group was five (out of a total possible of eight). Seven participants commenced only one or two modules, and eight participants commenced all eight modules. Of the 123 modules commenced in total, the majority (87.8%) were 100% complete. In terms of the activities associated with each module, participants completed an average of eight out of a total possible of 16 activities each. The message board was only used by six participants; five participants used it once and one participant used it twice. The message board was exclusively used to communicate about practical difficulties accessing the modules.
A proportion of participants reported receiving treatment from a psychologist at the 10-week assessment (52% of control and 58% of Reframe-IT participants). A smaller proportion was seeing a psychiatrist (0% control; 16% Reframe-IT), a counsellor (14% control; 11% Reframe-IT), a social worker (5% control; 0% Reframe-IT) or a headspace clinician (43% control; 5% Reframe-IT). Fourteen per cent of participants in the control group and 32% of participants using Reframe-IT reported being on medication at the 10-week assessment.
Outcomes
Analysis was by original assigned groups. There was an improvement in the mean scores for each symptom measure from baseline to 10-week and 22-week follow-up for participants in both intervention and control groups (see table 2). Suicidal ideation (SIQ) scores decreased to a greater extent in the intervention group compared with the control group from baseline to 10-week follow-up (intervention −37.3, SD 39.1 vs control −31.6, SD 42.8; 39 participants overall) and from baseline to 22-week follow-up (intervention −61.6, SD 41.6 vs control −47.1, SD 42.3; 30 participants in total). Although the mean decrease in suicidal ideation was larger in the intervention group compared with the control group, the differences were not statistically significant (p=0.593).
At the 10-week follow-up, none of the participants in the intervention group reported any suicide attempt since the baseline assessment. This is compared with three participants in the control group who reported a total of nine suicide attempts. At the 22-week assessment, none of the intervention participants reported a suicide attempt since the 10-week assessment, compared with two participants in the control group who reported a total of four suicide attempts. The differences between groups were not significant at any time point.
Self-reported depression severity (RADS) decreased to a greater extent in the intervention group compared with the control group from baseline to 10-week follow-up (intervention −4.8, SD 7.8; control −3.5, SD 4.8) and from baseline to 22-week follow-up (intervention −9.5, SD 6.3; control −6.4, SD 7.3). Clinician reported depression severity (CDRS-R) decreased to a greater extent in the intervention group compared with the control group from baseline to 10-week follow-up (intervention −9.2, SD 15.6; control −5.4, SD 16.9) and from baseline to 22-week follow-up (intervention −16.1, SD 14.9; control −11.2, SD 19.3). Hopelessness (BHS) decreased to a greater extent in the intervention group compared with the control group from baseline to 10-week follow-up (intervention −1.8, SD 4.2; control −1.7, SD 5.7) and from baseline to 22-week follow-up (intervention −4.8, SD 4.1; control −4.2, SD 6.2). Anxiety severity (MASC) decreased to a greater extent in the intervention group compared with the control group from baseline to 10-week follow-up (intervention −9.6, SD 14.9; control −4.6, SD 14.0) and from baseline to 22-week follow-up (intervention −13.2, SD 21.8; control −7.8, SD 13.6). Negative problem orientation (NPOQ) decreased to a greater extent in the intervention group compared with the control group from baseline to 10-week follow-up (intervention −5.3, SD 12.6; control −3.8, SD 8.4) and from baseline to 22-week follow-up (intervention −10.9, SD 13.1; control −5.8, SD 7.8). Cognitive behavioural skills (CBTSQ) increased to a greater extent in the intervention group compared with the control group from baseline to 10-week follow-up (intervention 6.1, SD 11.8; control 0.4, SD 10.3) and from baseline to 22-week follow-up (intervention 6.9, SD 8.0; control 1.8, SD 8.9). More specifically behavioural skills (CBTSQ-BA) improved to a greater extent in the intervention group compared with the control group from baseline to 10-week follow-up (intervention 2.9, SD 5.2; control 2.2, SD 5.2) and from baseline to 22-week follow-up (intervention 4.4, SD 6.7; control 3.1, SD 4.7). For cognitive skills (CBTSQ-CR), the intervention group improved from baseline to 10-week follow-up (intervention 3.1, SD 9.7); however, the control group deteriorated (control −1.8, SD 6.9), with a similar pattern from baseline to 22-week follow-up (intervention 2.5, SD 5.9; control −1.2, SD 6.2). Although the mean improvement in the intervention group was larger than that in the control group for all outcome measures, none of the differences between groups were significant (see table 2).
Distress
There were a total of 90 ‘before’ and ‘after’ module ratings of suicidal ideation, with 20 ratings for module one, reducing to four ratings for module eight. For the vast majority of module ratings, there was no change in the level of suicidal ideation, rated on a scale of 0 to 3, after viewing the modules (68/90, 75.5%). Most of the module ratings indicated there was no suicidal ideation before or after completing a module (n 55 module ratings, with 11 indicating mild suicidal ideation before and after and 2 indicating moderate levels of suicidal ideation before and after.) Just over 14% of module ratings indicated an improvement in suicidal ideation after completing a module (13/90, 14.4%; 10 module ratings indicated a drop from mild to no suicidal ideation; three module ratings indicated a drop from moderate to mild levels of suicidal ideation). A total of nine module ratings (9%) indicated an increase in suicidal ideation after completing a module; six of these module ratings indicated an increase from no suicidal ideation to mild levels of suicidal ideation, and three module ratings indicated an increase from mild to moderate levels of suicidal ideation. There was no particular pattern with regard to which modules were associated with increases in suicidal ideation, but this is difficult to establish with such low numbers of module ratings indicating an increase in suicidal ideation.
Mediation analysis
Table 3 shows the correlations between changes in various symptom measures and mediator variables from baseline to 10-week follow-up. There were several correlations that satisfied the test of mediation. These showed that changes in depression partly mediated the impact of the acquisition of CBT skills generally and behavioural skill specifically on suicidal ideation, and that changes in hopelessness partly mediated the impact of the acquisition of CBT skills generally on suicidal ideation.
Correlations of changes between symptom measures and mediator variables between baseline and 10-week follow-up
Discussion
We conducted an RCT of an online CBT intervention (Reframe-IT) for young people with suicide-related behaviours to which we were only able to recruit 50 of the planned 169 participants. We observed improvements in suicidal ideation, frequency of suicide attempts, depression, hopelessness, anxiety and problem solving ability in both the intervention and control groups. Although the improvements were larger in the intervention group, indicating the intervention is potentially efficacious, there were no statistically significant differences between groups. Importantly, there were no increases in suicidal ideation generally over the course of the study, or after completion of each module, among the majority of participants, hence indicating that the intervention is safe to administer. There were procedures in place to ensure the safety of those participants whose suicidal ideation did increase. Results are consistent with our pilot study of this intervention that showed that distress did not increase as a result of completing each module in the majority of participants.16 Further, the message board was used appropriately. A deliberate decision was made not to include any social networking functionality in the program due to concerns about ethical issues such as confidentiality and duty of care if a young person expresses suicidal ideation on a professionally run platform26 27 and fear of contagion.28 However, inclusion of social networking in a manner that is safe and supportive appears to be a logical next step given it may improve social connectedness, a known protective factor for suicide attempt.29 These findings give us some confidence that there are safe ways for professionals to engage with suicidal young people via online platforms. This is important given the increase in the use of online platforms by young people and the fact that better integration of online platforms into clinical care is increasingly advocated for.30
Participants appeared to benefit from the intervention in terms of increased use of CBT skills, with those in the intervention group using cognitive and behavioural skills more so than those in the control group. Given the differences were not significant, it is difficult to draw firm conclusion; however, there was an association between use of CBT skills and symptom improvement. Mediation analysis showed that the acquisition of general CBT skills, as well as behavioural skills specifically, was associated with an improvement in depression, which was in turn associated with an improvement in suicidal ideation. The acquisition of general CBT skills was also associated with an improvement in hopelessness, which was in turn associated with an improvement in suicidal ideation. This may suggest that teaching young people cognitive and behavioural skills is a good approach in reducing the symptoms we know are associated with suicidal ideation.
Study limitations
The main limitation of this study is the lack of statistical power given the recruitment rate was too low to meet sample size requirements. It is not uncommon for trials in the field of suicide prevention to be underpowered. There were difficulties with recruitment into the study, which was undertaken via school welfare staff. While young people see school welfare staff as an acceptable source of help, there is a range of reasons why they might not seek help and a range of reasons why school welfare staff may not feel confident about referring young people into a research study. This included the fact that school welfare staff are extremely busy, particularly in the context of complex but necessary (given safety issues) recruitment and consent processes that included the requirement for parental consent. Given often significant levels of suicide risk, school welfare staff were often reluctant to introduce the idea of research to students and were unsure about whether to include yet another intervention for those already receiving a range of services. The other consideration is that TAU was received by all of the participants in the trial, which included contact with the school well-being staff, as well as interventions by various mental health professionals outside of school. As a result, it may be difficult to detect an effect of a relatively benign intervention such as Reframe-IT over and above the effects of active face-to-face clinical treatment. Often this additional intervention received as part of TAU was the result of referral on the basis of the baseline assessment, highlighting the potential benefit of this type of intervention for facilitating access to mental health services.
There was also a high dropout rate (50% in the intervention group and 29% in the control group by 22-week follow-up), which resulted in large amounts of missing data for outcome measures, particularly the measure of CBT skill acquisition.
Results may only be generalisable to help-seeking young people with suicide-related behaviours given this is how young people were recruited to the trial; the participants in this trial also had significant depression symptoms. Along with a small sample size, this means that the study findings may not be generalisable.
Notwithstanding these limitations, this novel trial used high-quality methods and was conducted in line with the Spirit guidelines31 and reported in line with the Consolidated Standards of Reporting Trials (CONSORT) guidelines.32
Clinical implications
This project was the first of its kind internationally, and importantly included young people with significant levels of depression, anxiety and suicidal ideation, many of who had a history of suicide attempts. Although it was difficult to recruit sufficient participants into the trial, those who did participate were safely and generally well engaged in Reframe-IT and experienced decreases in suicidal ideation and other symptoms. Demonstration of the feasibility of safely including suicidal young people in a trial is a significant advance in knowledge for the field given young people at risk of suicide are typically excluded from mental health intervention trials.33 Researchers should feel more confident about undertaking research with young people who are at risk of suicide, as long as appropriate protocols for managing risk are included. As such, this study paves the way for a new generation of suicide prevention research. Increasing knowledge in this area, including understanding the mechanisms by which interventions reduce suicide risk, is critical given the relative paucity of evidence-based interventions for this population. Prevalence rates of suicidal ideation and suicide attempts are high, and services, such as school welfare services, often struggle to manage demand. Interventions like Reframe-IT provide a potential additional resource that can be used with students at risk of suicide. It may be that future research uses a more direct approach to recruit participants rather than recruitment via school welfare staff who are in contact with young people.
Acknowledgments
We wish to thank the schools for their participation, and especially the young people who took part in the trial. We also wish to thank String Theory for the technical development of the online platform to house the intervention written and designed by JR and SH.
References
Footnotes
Funding The study was funded by beyondblue, an Australian organisation that aims to improve mental health literacy and decrease stigma, that also provides research funding, in the area of depression, anxiety and suicide prevention. JR is on an NMHRC Early Career Fellowship and SMR is supported by the Mary Elizabeth Watson Early Career Fellowship from Royal Melbourne Hospital.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.