Article Text

Abstract
Background Currently, there is no accepted system for the classification of psychotherapies for application within systematic reviews. The creation of anuncomplicated, understandable and practical classification system is neccessary for conducting reliable systematic reviews.
Objective To devise a system for classification of psychotherapy interventions—for use, initially, in systematic reviews.
Methods Cochrane Schizophrenia’s Register used as the source of randomised controlled trial. After being piloted and refined at least twice, finally we applied it to all relevant trials within the register. Basic statistical data already held within the register were extracted and used to calculate the distribution of schizophrenia research by form of psychotherapy.
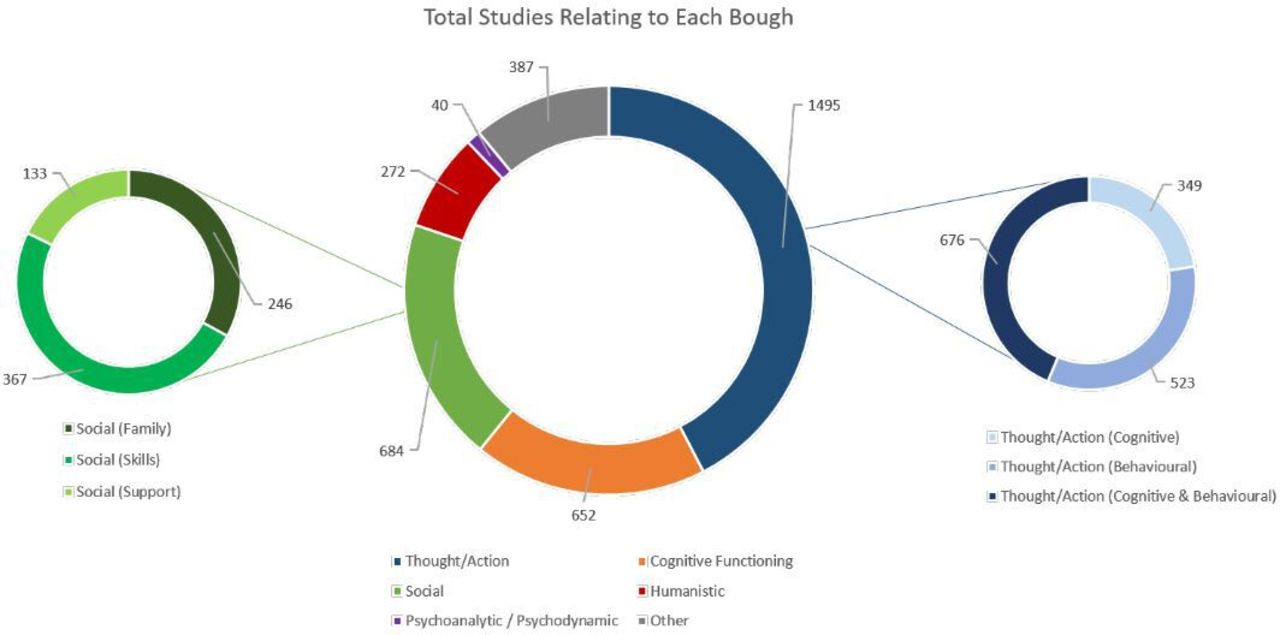
Findings The final classification system consisted of six definable broad ‘boughs’ two of which were further subdivided into ‘branches’. The taxonomy accommodated all psychotherapy interventions described in the register. Of the initial 1645 intervention categories within the register, after careful recoding, 539 (33%) were psychotherapies (234 coded as ‘Thought/Action’ (cognitive & behavioural)—1495 studies; 135 ‘Cognitive Functioning’—652 studies; 113 ‘Social’—684 studies; 55 ‘Humanistic’—272 studies; 23 ‘Psychoanalytic/dynamic’—40 studies; and 63 ‘Other’—387 studies). For people with schizophrenia, across categories, the average size of psychotherapy trial is small (107) but there are notable and important exceptions.
Conclusion We reported a practical method for categorising psychotherapy interventions in evaluative studies with applications beyond schizophrenia. A move towards consensus on the classification and reporting of psychotherapies is needed.
Clinical implications This classification can aid clinicians, clinical practice guideline developers, and evidence synthesis experts to recognise and compare the interventions from same or different classes.
- schizophrenia & psychotic disorders
- adult psychiatry
- child & adolescent psychiatry
- delirium & cognitive disorders
- forensic psychiatry
Data availability statement
The full database of intervention categories analysed in this study is available from the authors on request.
Statistics from Altmetric.com
- schizophrenia & psychotic disorders
- adult psychiatry
- child & adolescent psychiatry
- delirium & cognitive disorders
- forensic psychiatry
Background
Accurate and systematic classification of medical interventions is integral to the practice of evidence-based medicine. Those compiling treatment guidelines often used randomised controlled trials (RCTs) as building blocks within systematic reviews.1 Comprehensive identification of RCTs is particularly important to ensure all relevant data are considered and random error and systematic bias minimised in the eventual syntheses.2 3 In addition, the development of a practical system of classification of psychotherapies would open novel avenues of research previously made difficult because of confusions of nomenclature.
Effective classification of medical interventions is a prerequisite for their accurate detection, description and grouping. Otherwise, similar treatments have to be identified by the diverse names assigned to them.4 Such classifications now exist for medications,5 but the dynamic nature of the field of psychotherapy, as well as the limited regulation in naming/description of interventions, presents challenges to production of a classification in this area.
Objective
To devise a practical system for classification of psychotherapy interventions for use, initially, in accurate identification of studies for relevant systematic reviews
As a secondary objective, to employ the new system to help describe frequencies and size of studies of all published schizophrenia psychotherapy RCTs
Methods
We attempted to arrive at a working definition of ‘psychotherapy’, sought classification systems of the past to use or adapt, piloted the initial attempt at a purpose-built classification on all relevant schizophrenia psychotherapy trials, and modified the system in line with this experience.
Definition
Existing definitions, sourced from past classifications (table 1), were considered and discussed with an academic psychologist (MG). These definitions are often intentionally broad and not formulated with classification in mind. In the definition we formulated for this work we aimed to capture the fundamentals of psychotherapy while creating something understandable, practical and systematic.
Psychotherapy—a working definition:
A treatment whose primary purpose is the improvement or prevention of direct psychological and mental sequelae of mental illness/psychopathology which:
Is intended to work primarily through interaction with the recipient’s mind, AND
Involves the active interaction of the recipient with the treatment, AND
Does not involve the external administration of a substance or physical effect to the recipient as its primary mechanism
Characteristics of previous categorisation attempts
This definition was formulated by synthesising existing definitions with examples of therapies found in the interventions we examined. Point 1 ensures that all psychological therapies are covered by the definition, while excluding certain therapies which, while not pharmacological in nature, are not primarily psychological in nature—such as exclusively physical and lifestyle/economic interventions. Point 2 establishes the principle that a therapy must be something the recipient engages with. It cannot, for example, simply be a change to the recipient’s circumstances—even if such changes are primarily intended to have a psychological benefit. We did not specify a requirement for a therapeutic relationship since some psychological therapies involve minimal or no focus on such a relationship—such as some forms of cognitive remediation, and therapies which are undertaken independently by the recipient without the presence of a therapist. Finally, point 3 excludes both pharmacological therapies, as well as interventions such as electroconvulsive therapy. These are intended to deliver a psychological benefit, but are not psychological therapies in of themselves.
Previous attempts at classification
No widely accepted systematic approach to the classification of psychotherapy interventions exists. Prominent forms of psychotherapy, such as cognitive–behavioural therapy (CBT), are widely recognised and grouped together through various informal groupings.6 However, the array of psychotherapies is vast and growing as practitioners develop novel methods. Many of these developments have names that imply overlap with past methods. However, despite similarity in nomenclature, many use different methods or theoretical underpinnings.
We sought past attempts at classification by bibliographic database searches and tabulated these. Table 1 is not a comprehensive list, but rather, outlines four overlapping but distinct perspectives we found particularly valuable. Unsurprisingly, we could not directly implement any of the previous attempts. None were designed with the specific purpose of assisting trial identification for systematic reviews.
Source of data: Cochrane Schizophrenia’s Study-Based Register of Trials
This register—started nearly 30 years ago—to facilitate the systematic review process (2) is now supported by the UK National Institute for Health Research (NIHR). It contains every report of every relevant randomised trial but, within it, a single study record is linked (related) to all relevant reports of that trial to help avoid multiple counting.7 Creation of unique study records affords opportunity to rationalise nomenclature—to classify. This has been the case for medications, and now metadata on medication interventions have a fully controlled language.5 This is not the case for other treatments and, currently, FS simply records the name of these other treatments verbatim from the study report with no categorisation. It is on this list of RCT-centric psychotherapy interventions the categorisation was piloted.
Creation of the initial classification
We used a methods-based approach, identified examples of each uniquely named psychotherapy from the register, and divided and categorised these by their purported method of action. Our efforts were guided by the pioneering work (outlined in table 1), the descriptions of interventions in trials and constant consideration of our primary objective—which was to produce a practical classification to aid reliable identification of relevant studies for reviews.
Stage 1: piloting
Our initial classification produced six reasonably distinct boughs off the main trunk of psychotherapy. These were possible to describe to aid information specialists assigning new studies to a bough. Any given study could be assigned multiple boughs.
The (initial) six boughs—with working definitions—were as follows:
Behavioural: ‘Developing different behaviours leads to change’.
Cognitive: ‘Changing thought patterns leads to change’.
Humanistic: ‘Empowering the patient leads to change’.
Psychodynamic/psychoanalytic: ‘Understanding of the self, past experiences, and the unconscious leads to change’.
Social: ‘Changing interpersonal/intergroup relationships leads to change’.
Other: psychotherapies that do not fit into any of the above categories, or contain an element which is not captured by any of the above categories.
Stage 2: modification
As piloting on samples of trials from the register progressed, some alterations to the classification were necessary. Principle among these were changes made to the behavioural and cognitive boughs. First, it was clear that two distinct groups fit under the umbrella of Cognitive interventions. One focuses on cognitive content and the other on cognitive functioning. ‘Content’ relates to what a person thinks about, whereas ‘Functioning’ involves emotion recognition, memory and other domains. To address this, we separated the Cognitive bough into two—Cognitive Content and Cognitive Functioning.
Second—and unsurprisingly given their shared epistemological history—there was considerable overlap between many Behavioural and Cognitive Content interventions. This was most pronounced for interventions which did not explicitly name themselves as ‘behavioural’ or ‘cognitive’, but which, in their description, clearly belonged to at least one of these boughs. Even for interventions explicitly identified with either Behavioural or Cognitive schools of thought, we found significant degrees of overlap in the actual methods used. To address this we grouped Behavioural and Cognitive Content together as subdivisions (branches) under a bough now termed Thought/Action. Where possible, we attempted to separate interventions into one of the two subdivisions—but such separation is frequently impossible.
During the process of creating the classification, we consulted with an academic psychologist, MG, who provided ongoing advice on the construction and definition of the classification for each bough of psychotherapy. This ensured that our classification had face-validity and was coherent with the understanding of psychotherapies held by professionals in the field.
Final categorisation:
Thought/Action (T/A): ‘Developing different behaviours and thought patterns leads to change’.
Subdivision: Behaviours: ‘T/A methods primarily orientated towards changing behaviours’.
Subdivision: Cognitive: ‘T/A methods primarily orientated towards changing thought patterns’.
Cognitive Functioning: ‘Improving cognitive functions and skills leads to change’.
Humanistic: ‘Empowering the patient leads to change’.
Psychodynamic/Psychoanalytic: ‘Understanding of the self, past experiences, and the unconscious leads to change’.
Social: ‘Changing interpersonal/intergroup relationships leads to change’.
Subdivision: Family: ‘Social methods based on altering family dynamics and relationships’.
Subdivision: Social Skills: ‘Social methods based on improving ability of patients to form, maintain, and use social relationships and networks’.
Subdivision: Social Support: ‘Social methods based on directly providing patients with supportive social relationships and networks’.
Other: psychotherapies which do not fit into any of the above categories, or which contain an element not captured by any of the above categories.
(for a more detailed description of each bough—see online supplemental appendix 1)
Supplemental material
Reclassification of intervention categories
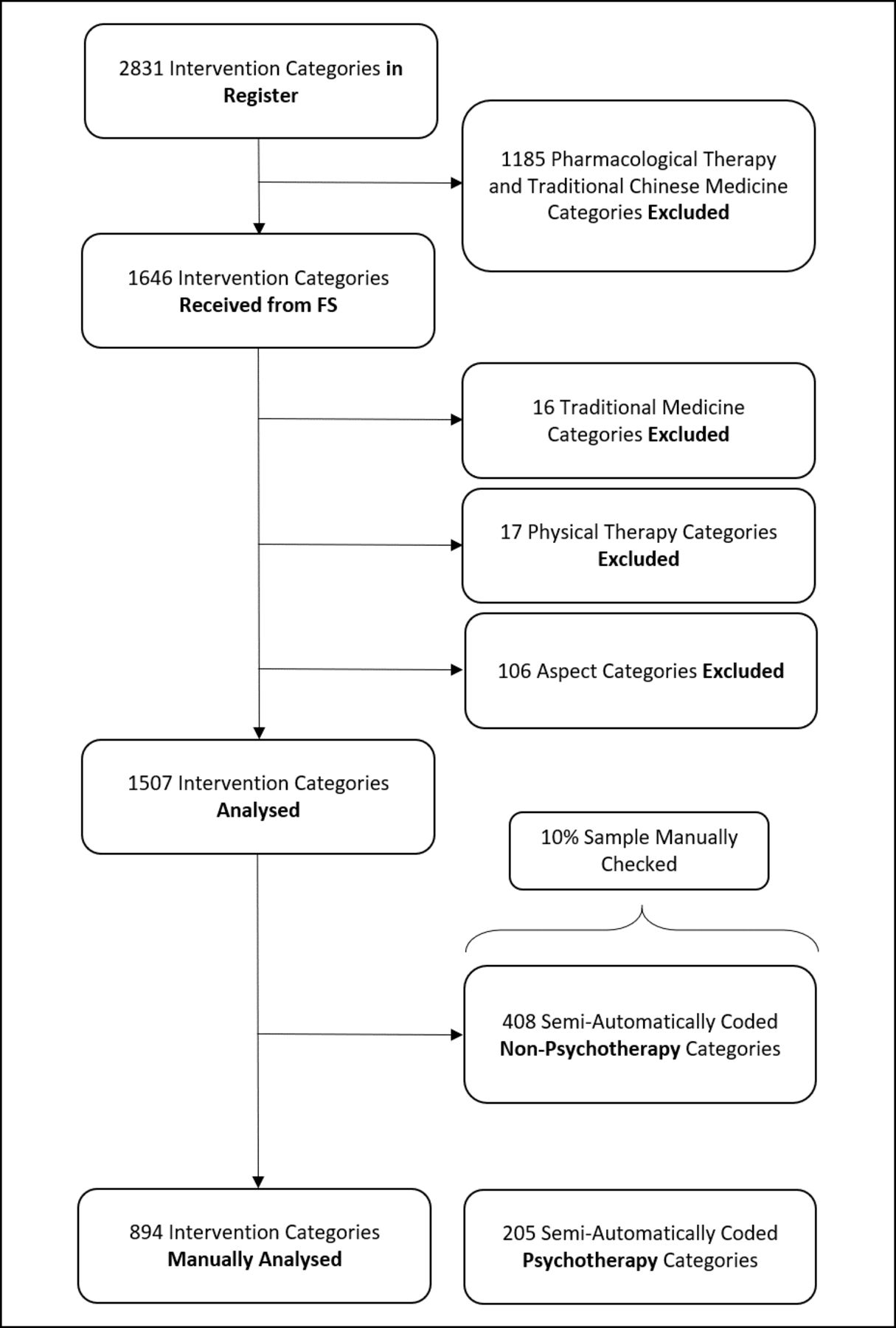
Having piloted and modified the classification using limited subsets of trials from within the Cochrane Schizophrenia register, we now applied the classification to the intervention categories of the whole register of randomised studies (for an explanation of the structure of the Cochrane register as relevant to this analysis—see online supplemental appendix 2). FS (information specialist) provided a version of the register having removed all pharmacological intervention categories and traditional Chinese medicine categories (see below) (leaving 1646 unique intervention categories). For purposes of utility, this version was then further streamlined so that each remaining intervention category appeared as a single instance (linked to a single key reference). However, a complete version of the database was preserved so that all studies, references and full text PDFs linked to a specific intervention category could be viewed if required.
Each intervention category was reviewed and, where necessary, recoded based on the classification as outlined above.
First pass: initially, we had to exclude traditional medicines, such as Ayurvedic and Traditional Japanese medicines. As with traditional Chinese medicines, which had already been excluded, these involve a physical treatment but may be accompanied by some manner of psychological approach. The descriptions of these interventions were limited, and further compromised by our understanding, rendering classification impossible. We realise that this could give our classification a bias towards a ‘Western’ paradigm.
We also excluded the ‘pure’ physical therapies as many did not fit our definition of psychotherapy. The exceptions were physical therapies with a specific clear theoretical underpinning based on one of the six bough categories (such as body psychotherapy and body awareness therapy, which have a psychodynamic/analytic underpinning).
Finally, we excluded those categories which described an ‘Aspect’ of treatment (categories which describe a generalisable aspect of an intervention rather than the intervention itself).
Second pass: we then considered the previous labelling of the studies—the intervention categories in the Cochrane trial register which had been unsystematically applied prior to the creation of this classification. Where this closely corresponded to the new classification, we reused these intervention categories without close examination of their linked reference(s). For example, the old intervention category ‘Psychoanalytic Psychotherapy’ clearly corresponded to the new ‘Psychoanalytic/Psychodynamic’ category.
A total of 205 intervention categories were coded as psychotherapy interventions using this ‘semi-automatic’ method. Using the same approach, a further 408 intervention categories were assessed, and judged not to correspond to a psychotherapy intervention—for example, ‘Transcutaneous Vagus Nerve Stimulation’.
As this process did not involve a full examination of every single linked reference for each intervention category, there was a risk of error. To address this, 10% of each of the two groups described above were randomly selected and fully examined to ensure that the process was reliable. For this manual rechecking, we accepted an accuracy rate of 80% and above (online supplemental appendix 3).
Third pass: the main coding pass. Again, each category was judged as to whether it described a psychotherapy intervention. If so, it was then coded to one or more relevant boughs. Where possible each intervention category was coded to one bough and, where possible, the ‘Other’ bough was avoided. Where intervention categories clearly corresponded to more than one group, however, this was reflected in the coding. We judged that sensitivity is preferable to specificity—for a reviewer conducting a meta-analysis using the Cochrane database to identify trials for inclusion it is far more important to minimise false negatives than false positives. Although it wastes time, the latter can be manually excluded.
Coding of each psychotherapy intervention was achieved through:
Examination of the single randomly selected example study; and if any doubt remained.
Examination of other studies linked to that intervention category in the unstreamlined database segment; and if doubt continues.
Consulting auxiliary sources (eg, (11), (7)).
See figure 1 for a breakdown of the process and number of intervention categories analysed through each classification pass. We have described this process in terms of number of intervention categories rather than studies, as that was the focus of this part of the method. Additionally, the wide variation in the number of trials related to each intervention category would render data related to the number of studies addressed in this process of limited value.
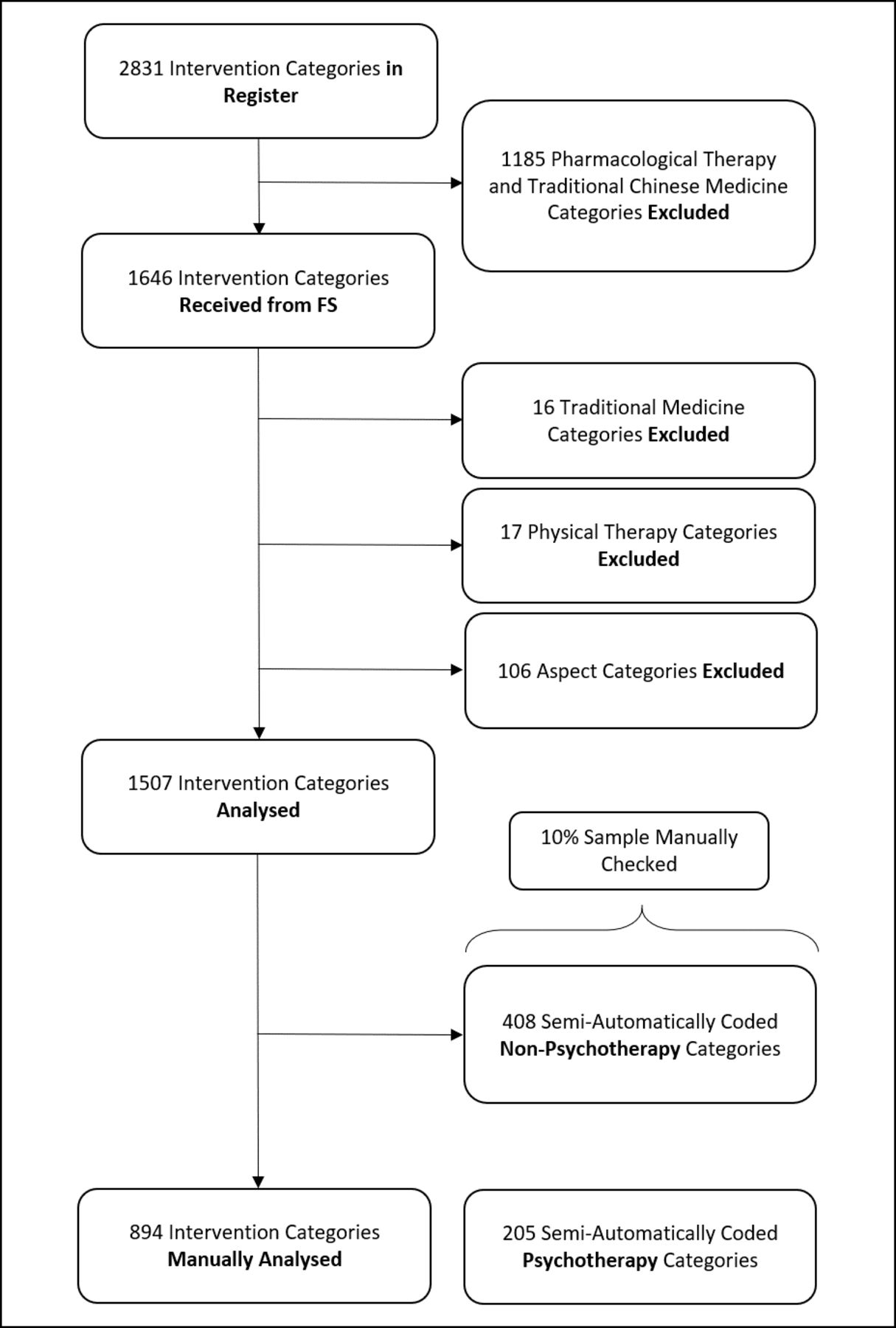
Selection of intervention categories for analysis.
Findings
One thousand five hundred and seven intervention categories were included in the analysis, of which 894 were analysed manually, while 613 were analysed using the semiautomatic method. The results for the full 1507 intervention categories are presented below.
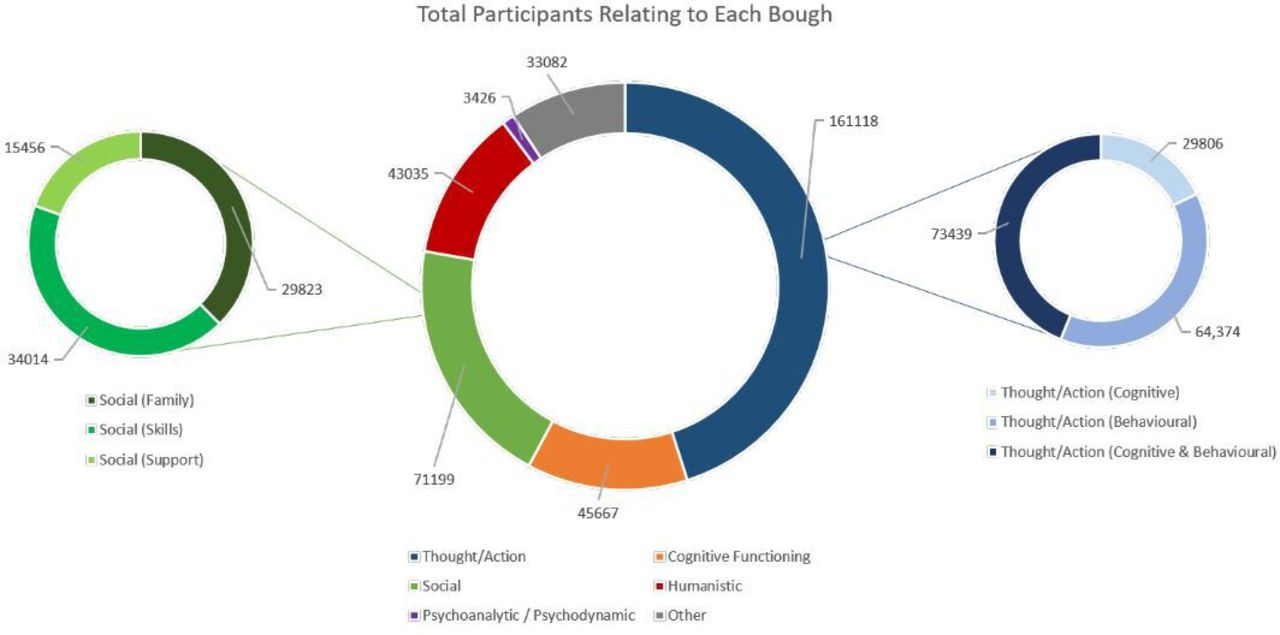
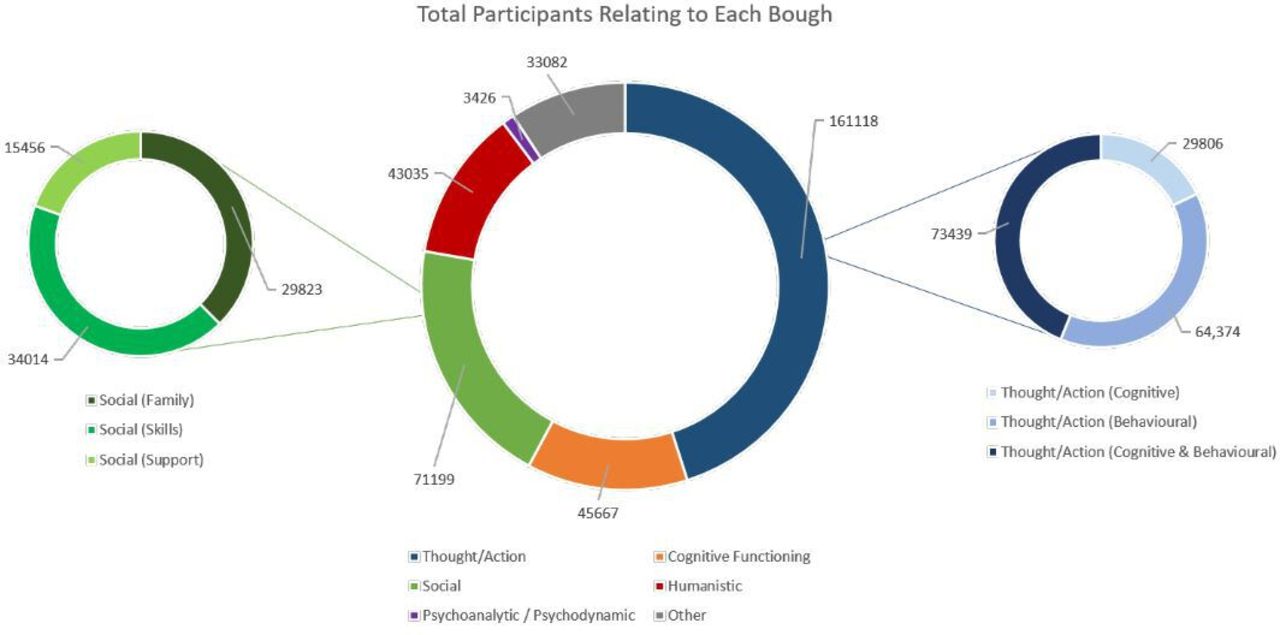
Following analysis, 539 intervention categories were judged to correspond to psychotherapy interventions. The distribution of these intervention categories, in terms of boughs, studies (Figure 2) and participants (figure 3), are summarised in table 2. Examples of intervention categories coded to each bough are presented in table 3. The full database of intervention categories analysed in this study is available from the authors on request. Thirty-eight intervention categories were coded as adjuncts, of which 18 were also coded as psychotherapies. Two hundred and thirty-six intervention categories were only linked to references in foreign languages. Of these, 230 were in a Chinese language, and were later analysed separately by a second researcher (YS), and are included in the analysis.
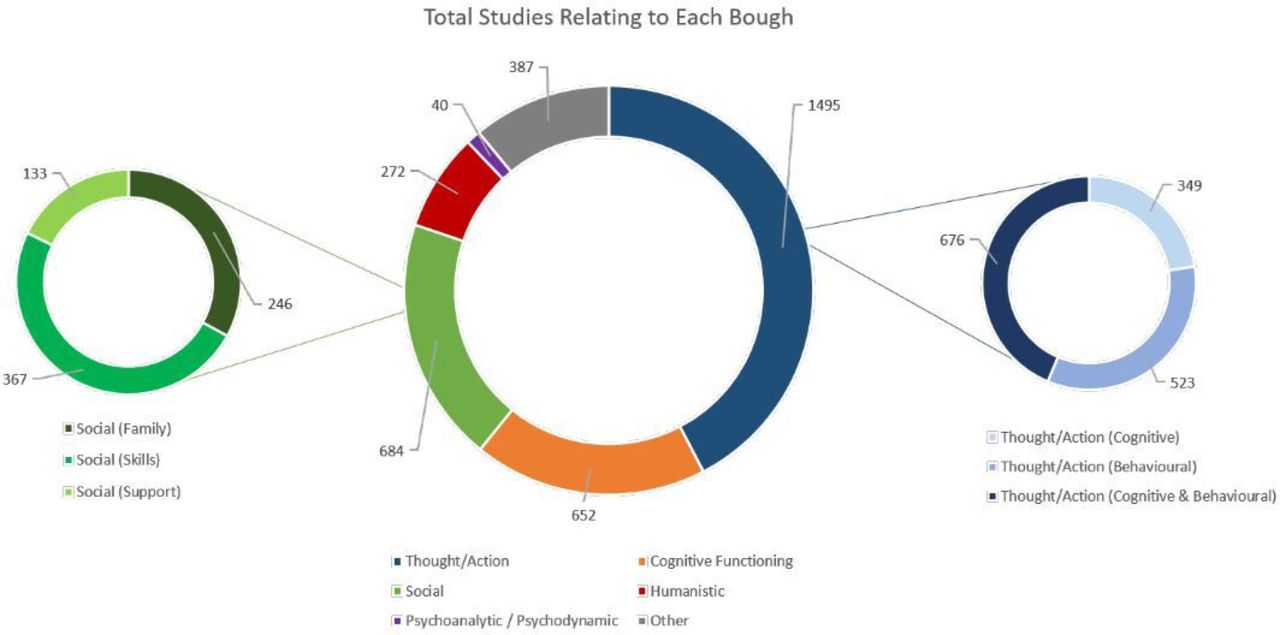
Total studies relating to each psychotherapy bough.
{kind=link}
{kind=link}
{kind=link}
Total participants relating to each psychotherapy bough.
Distribution of analysed intervention categories (primary analysis)
Examples of intervention categories coded to each Bough
Several of the 894 categories were eventually coded as ‘delivery methods’. They are not psychotherapies, instead they represent the way in which a person may become exposed to a psychotherapy. For instance, ‘Assertive and Outreach Support Teams’ can deliver various forms of interventions—including psychotherapies—but this intervention is not itself a psychotherapy.
Similarly, several intervention category categories were coded as ‘adjuncts’—meaning they do not necessarily represent a ‘school’ of psychotherapy but may be used in therapy to support any form of psychotherapy. We defined adjuncts as a method of therapy designed to facilitate/complement the delivery of a psychotherapy, and, typically, one that is not used as a stand-alone psychotherapy. However, one identically named intervention could be an adjunct in one trial, and a psychotherapy in a second study. For example, art therapy can be used in a psychoanalytic manner, or can be used as an adjunct or delivery method of other therapies. Where we felt that adjuncts may also be argued to be a form of psychotherapy in themselves, we also coded them as such. We recognise that many of these therapies are still emerging, and theoretical bases are evolving. We therefore welcome and invite feedback from practitioners of these therapies for how we can better categorise them.
Discussion
Separating the boughs
We regard an ideal classification system for use in systematic research as one which strikes a balance between:
Practicality/applicability: able to be quickly understood and easily applied to practical purposes.
Recognisability: uses existing terms that are common in the psychological lexicon.
Simplicity: avoids unnecessary introduction of layers of complexity, subdivisions, or fine-grain separating of similar categories, where these elements do not serve a practical purpose.
This classification is applicable to interventions in studies in the Cochrane Schizophrenia Register and all were able to be categorised based off a relatively rapid assessment of any given study. We were encouraged that a relatively small number of psychotherapy intervention categories needed to be coded as ‘Other’ (over 90% of psychotherapy interventions were given a label that specifically described their ‘mechanism’). Furthermore, our classification was largely consistent with those described in past work.8–10 While ours is distinct by virtue of its basis in literature rather than clinical practice, the high consistency suggests that arrival at a consensus on common language for psychotherapy classification is within reach. Achieving this goal required creation of clear, recognisable boughs, with minimal introduction of new terminology and as much reference as possible to current understanding of the subdivisions.
In the simplest case, each psychotherapy would be assigned to a single bough, and hence be described by a single code. In practice, however, many interventions represent syntheses and combinations of theories and techniques and it would be too reductive to describe them as belonging to a single bough of the tree of psychotherapy. We, therefore, accepted the need for the possible assignment of an intervention to multiple boughs of psychotherapy and feel this approach is the most coherent with the reality of psychotherapeutic practice. Moving forward, there may be value in the development of a weighting system allowing quantitative estimation of the degree to which a ‘multi-bough’ intervention corresponds to each branch of psychotherapy.
The boughs and branches must be dynamic. So long as researchers and practitioners provide clear theoretical and mechanistic frameworks for their approaches, the existing boughs should remain valid as novel therapies become established. However, once reliably coded, such classification lends itself to the capacity for swift reconsideration of the configuration of the whole tree—including the possibility of creation of new boughs/branches.
Distribution of schizophrenia psychotherapy studies
The average size of psychotherapy trial for people with schizophrenia is small (107), with little variation in size between different the boughs. These trials will have limited statistical power.11 However, the existence of several trials in each bough with sample sizes considerably larger than the mean, demonstrates the feasibility of conducting much more powerful studies. In the future, there would be benefit in more large, high quality, collaborative studies, achieving sample sizes of real power to investigate outcomes of importance to clinicians and recipients of care. It would also be of benefit to those classifying such studies.
The most researched psychotherapy in schizophrenia care is CBT. Although the above issue of sample size does apply, this group of researchers have invested much effort testing the effects of these approaches. The clarity of description was good enough to make grouping these trials easy and this greatly facilitated producing the relevant systematic review. There is a comparative lack of research into other areas of psychotherapy—in particular humanistic and psychoanalytic therapies. Given the very modest—if any—benefit of CBT in comparison to other psychotherapies for schizophrenia,12 this investment of research, clarity of description, ease of classification and supply, should allow researchers to move swiftly on to adaptions or other therapies that could be more effective.
The brief analyses presented are small and easy examples of what can be undertaken once confidence is increased in a clear classification system. Important and novel insights can be generated into research practice once classification is established, trusted and adhered to, preferably within a study-based register.
Recommendations for research
Journal editors could encourage authors of trials of psychotherapy to adhere to the Template for Intervention Description and Replication (TIDieR) checklist for intervention description and replication,13 with particular emphasis on Items 2 and 3 (‘Why?’ and ‘What?’). This will increase consistency and clarity of their descriptions of psychotherapies. To strengthen the TIDieR checklist when specifically applied to psychotherapy researchers, authors should clearly—and wherever possible in simple, jargon-free language—identify:
The school(s) of psychotherapy to which they feel the intervention belongs to; and
The theoretical underpinnings of the intervention, including—if applicable—the progenitor psychotherapies from which it developed; and
A comprehensive description of the practical steps involved in delivery of the intervention; and
The specific change in a patient’s condition the intervention is intended to produce, and the intended mechanism by which the described practical steps might achieve this.
We feel that while this classification system was generated by work on our schizophrenia-specific register, it could be used in any register of psychotherapy literature. Information specialists whose role involves evaluation of psychotherapies would greatly enhance evolution of classification by adoption of one workable system. We also invite feedback from academic and clinical professionals involved in schizophrenia psychotherapies, in order to further refine the classification.
Next steps
First, for Cochrane Schizophrenia, the register of studies will be updated with the new improved indexing categories and ‘live’ tested. This is not difficult as the register is in a MS Access database that can be updated with ease. This new indexing will be mapped onto Cochrane Schizophrenia’s publicly available topic tree,14 and in turn, relevant reviews attached to the ends of that tree. Live testing will then take place as new studies and references are added to the Cochrane Schizophrenia Register and reviews into the topic tree. Part of this ‘live testing’ will be the more detailed addition of trials not published in English. The register covers any language. In this paper, the large numbers of studies in Mandarin have been accounted for but there remain some trials the detail of which remains inaccessible to us because of language barriers.
Subsequently, it will be possible to use this classification to conduct more sensitive and specific reviews. In particular, the more accurate and systematic identification of the bough of psychotherapy to which a given intervention belongs will, for the first time, allow comprehensive reviews of that bough to be carried out. For instance, a researcher wishing to conduct a systematic review into the effectiveness of psychodynamic interventions can use this classification to easily and systematically identify which studies relate to such interventions. For boughs, we have subdivided into ‘branches’ (eg, the Family branch of Social); there is a further potential to conduct reviews of these specific divisions of given boughs. Using this system, the issue of heterogenous and inconsistent nomenclature for schizophrenia psychotherapy interventions can be easily remedied by applying the classification to a brief review of each paper considered. While we encourage researchers conducting RCTs to explicitly identify and explain which bough of psychotherapy their intervention is associated with, a strength of our classification is that in the absence of such author-led identification, reviewers are able to use the classification to quickly and systematically classify RCTs to boughs of psychotherapy independently.
This system of classification can be applied manually in any research setting, and indeed potentially in clinical settings, but will be most effective when used in concert with the Cochrane register of schizophrenia RCTs. This register has the benefit both of representing a comprehensive and continuously updated database of all schizophrenia RCTs, and—after the update of the register—of already having the classification incorporated into its coding. This will allow all RCTs for a given bough or branch to be retrieved at the touch of a button.
In future, there is potential for further subdivision of boughs into (more) ‘branches’ and ‘twigs’ (subdivisions of branches). Further analysis of each bough—and collaboration with researchers who have already attempted subdivisions of boughs and branches—should allow incorporation of increasing levels of specificity into the classification. Examples might include subdivision of Cognitive Functioning interventions by their targeted modality, subdivision of Humanistic interventions by their different forms, and further subdivision of the cognitive and behavioural subdivisions of Thought/Action interventions.15
Conclusion
The Nottingham classification of psychotherapies is a practical, understandable and comprehensive classification of the different boughs of psychotherapy. It is rooted in past classifications but, because its primary purpose was to allow for more accurate searching for systematic reviews of treatments, it has been primarily generated from scrutiny of existing literature.
Testing has begun on the classification and some insights into conduct of trials in this subspeciality have already emerged. Most relevant trials are too small to be truly informative, necessitating systematic reviews for synthesis of all evidence. However, larger studies with power to investigate outcomes meaningful to routine care are clearly possible—although such trials are rare.
Application of this classification to Cochrane Schizophrenia’s register of trials will facilitate more sensitive and specific searches and allow further testing and evolution of the system. Adoption beyond this important but specific register would help validate its broad value and addition of useful finer grain categories increases its sophistication.
In the longer term, it is vital that researchers, stakeholders and professional organisations actively move towards global consensus on common language and classification of psychotherapeutic interventions.
Data availability statement
The full database of intervention categories analysed in this study is available from the authors on request.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @FarhadShokrane
Contributors MTR has developed the protocol and ran the research and wrote the first draft of the manuscript and revised it. FS has developed the register, contributed in finding existing relevant classification literature, read the manuscript and made comments and prepared the manuscript for submission. YS contributed in refining the classification from a sample of trials and Chinese studies, double checking the classed and read and commented on the manuscript. MG research and commented on the classification and manuscript. CEA suggested the idea for this research and supervised the team on running this research. He read, commented and revised the manuscript several times.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.