Article Text

Abstract
Current education and training in psychological interventions is mostly based on different ‘schools’ (traditions such as cognitive–behavioural or psychodynamic therapy), and strong identification with these specific traditions continuously hinders a scientifically based development of psychotherapy. This review is selective rather than systematic and comprehensive. In addition to the consideration of other influential publications, we relied on a literature search in Web of Science using the following terms (update: 24 December 2020): (psychotherapy AND meta-analy* AND competence*). After summarising current problems, a pathway for solving these problems is presented. First, we have to recategorise psychological interventions according to the mechanisms and subgoals that are addressed. The interventions can be classified according to the foci: (1) skills acquisition (eg, communication, emotion regulation, mentalisation); (2) working with relationship patterns and using the therapeutic relationship to modify them; and (3) clarification of motives and goals. Afterwards, the training of psychotherapists can switch from focusing on one theoretical framework to learning the different competences for modification according to these new categories. The selection of topics to be addressed should follow best evidence-based mechanisms and processes of mental disorders and interventions. Psychology offers knowledge about these mechanisms that can be understood as a basic science for psychological treatments in general. This requires better connection with basic science, new research efforts that focus on treatment subgoals, theory-overarching optimisation of the selection and personalisation of treatments, and new types of training for psychotherapists that are designed to optimise therapists’ competences accordingly, instead of limiting training programmes to one single theoretical framework.
- adult psychiatry
- depression & mood disorders
Data availability statement
No data are available. No data included in this manuscript.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Psychotherapy is strongly categorised according to traditional roots (‘schools’), now being extended with new developments that continue to advocate one primary theoretical framework. This started with Freud’s outline of psychoanalysis and its emphasis on unconscious conflicts, with early behavioural therapy as a countermovement emphasising the role of observable behaviour, and subsequent innovations introducing own theoretical frameworks in their approaches (eg, acceptance, mindfulness, mentalisation, schemas). Consequently, in many countries, a typical education and training programme for young psychotherapists follows one of these theoretical frameworks.1 2 Healthcare systems and legal regulations for psychotherapy generally have continued to use the traditional categories.1 However, several problems arise from this orientation on one theoretical framework. This manuscript summarises the main problems that arise from the current situation of ‘school-based’ training in psychotherapy, and presents different perspectives for overcoming this stage of non-communication between advocates of the treatment approaches.
Methods
This review is selective rather than systematic and comprehensive. In addition to the consideration of other influential publications, we relied on a literature search in Web of Science using the following terms (update: 24 December 2020): (psychotherapy AND meta-analy* AND competence*). A summary of problems with the current psychotherapy training is provided. As a source for this summary, the corresponding scientific results and empirically based feedback from practice are used.
Problematic issues with current psychotherapy training
Psychotherapists often develop a strong identity and preference for one particular orientation, even if this is typically not fully supported by the empirical evidence. One consequence in science is the very obvious bias in reporting treatment results. Munder et al conclude that the difference in the effect sizes of similar treatments that can be attributed to investigators allegiance is d=0.54.3 Biased reporting of study results represents the deception of colleagues and of political stakeholders, and finally leads to unfounded treatment recommendations for patients. Psychotherapy research makes its own contributions to the replication crisis.4 Further problems are the neglect of perception and consideration of research-based disorder mechanisms, intervention tools and treatment processes that are not part of the favoured theoretical framework. Goldfried5 6 describes the field of psychotherapy as being in a prescientific development stage (‘over 100 years old, but still an infant science’). One characteristic of this stage is the lack of a common language and the lack of serious attempts to develop the overall subject of psychotherapy, instead of developing singular approaches.
The current education and training systems in psychotherapy have the unspoken assumption that a good psychotherapist is one who is expert in one psychotherapeutic tradition and one theoretical framework. The British psychoanalyst Fonagy, however, summarises that ‘recent studies indeed suggest that adherence flexibility (the capacity of the therapist to flexibly adapt treatment to the patient, which may involve using interventions from other treatment approaches and modalities) may be associated with superior outcomes’.7 Yet, we do not have an acknowledged framework for how and when this switch to other treatment approaches should take place, how integration of different approaches can be evidence based, and how to teach psychotherapists when and how to integrate the approaches of other theoretical frameworks.
Another negative consequence of focusing on one single theoretical framework is the neglect of identifying and integrating scientifically proven mechanisms and processes of mental disorders and change, emphasising exclusively the postulated and selective theory-conforming mechanisms. Therefore, Wampold and Imel 8 defined a counterposition emphasising more general principles of change. Accordingly, it is not the specific assumptions of the single therapy approach that explains successful treatments, but the so-called ‘common factors’. Although the distinction between common and specific factors should not be overemphasised, there are many relevant competences of psychotherapists, that are beyond the theory-specific assumptions.
What are the necessary competences of psychotherapists?
There is some light in the darkness of the psychotherapy world. When experts have to define the crucial competences of successful psychotherapists, surprisingly they come up with solutions that have only a few specific points from selected traditional frameworks,9 10 but they share many common features (box 1). Therefore, the ‘prescientific stage of psychotherapy’6 can be overcome by searching for a common umbrella that fits all evidence-based treatments. These competence lists associated with successful treatments should also consider the requirements of general society with all its stakeholders. The societal task of clinical psychologists and psychotherapists is not just to advocate and deliver one single treatment tradition, but also to have broad expertise and state-of-the-art scientific knowledge of the field.
Competence profile of clinical psychologists and psychotherapists according to European standards9
Psychotherapists are experts in the following fields:
General Psychological Processes in Health and Disease.
Mental and Behavioural Disorders and Psychological Processes in Physical Disorders.
Psychological Diagnostics.
Intervention: General Aspects.
Prevention, Rehabilitation: General Academic Expertise.
Scientific Methodology.
Ethical and Legal Aspects.
Skills for Psychological Interventions: Meta-Competences.
Skills for Psychological Interventions: Disorder-Specific, Person-Specific and Context-Specific Diagnostics and Interventions.
Skills for Psychological Interventions: Prevention, Rehabilitation.
Skills for Psychological Interventions: Setting-Specific Interventions, Modern Technologies.
Skills for Psychological Interventions: Documentation, Evaluation.
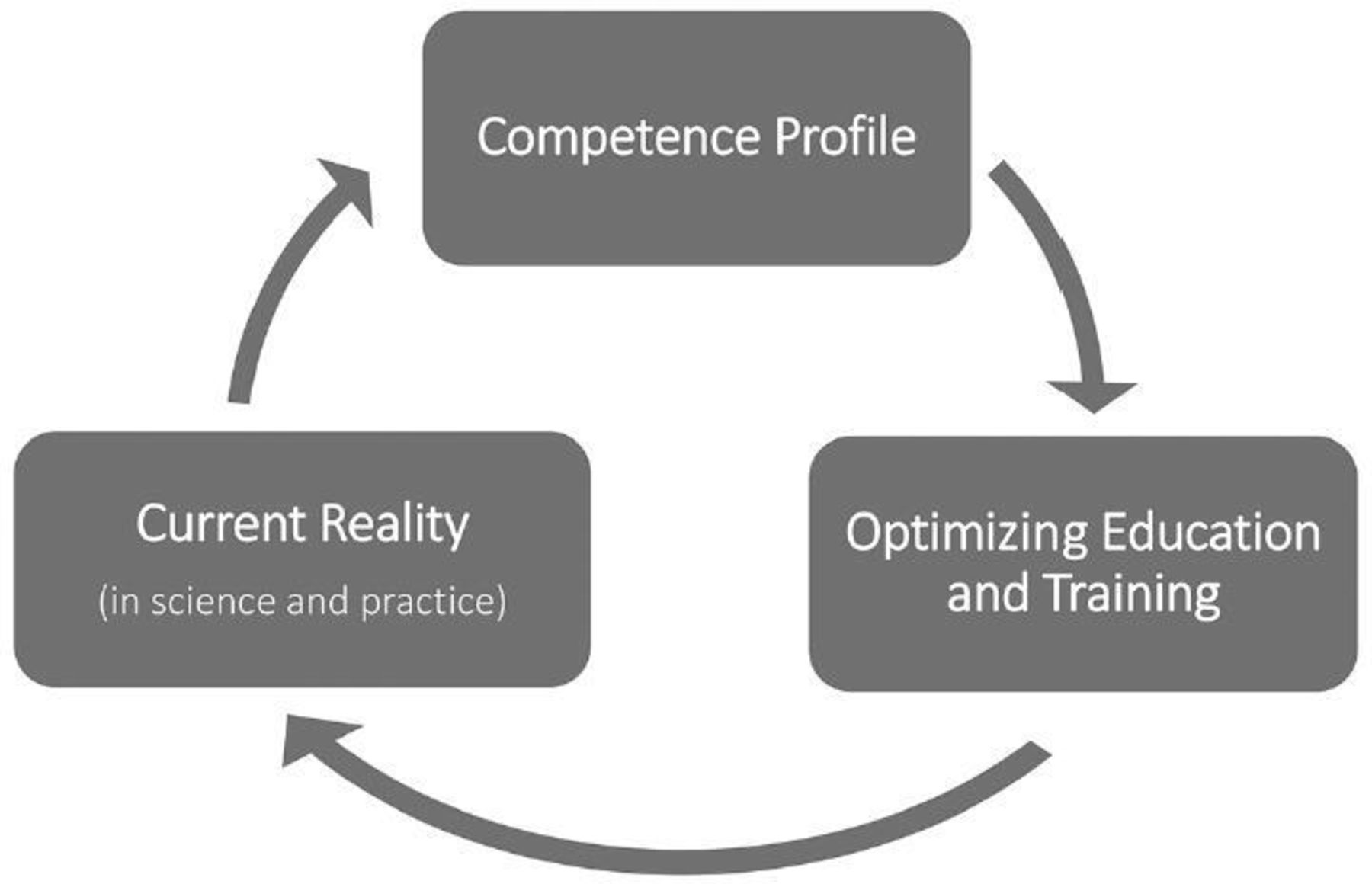
Furthermore, psychotherapists are requested to have not only academic but also personal competences,11 12 such as communication skills, empathy, mentalisation skills and emotion regulation skills, that are pivotal for successful work. Therefore, a competence-oriented framework can offer a pathway to an overarching theory of psychotherapy, that helps not only to integrate current existing and successful approaches but also common mechanisms and personal competence. Because a common language is needed for communicating in our field, we also have to identify core mechanisms of mental disorders and analyse how existing interventions address these core mechanisms. We also have to identify and focus on the core processes of successful intervention periods, and investigate variations of them experimentally, instead of exclusively evaluating full treatment packages. All this can form the basis of more personalised treatment planning and still consider research-based approaches. Then we can implement all this knowledge and integrate the relevant competences in revised versions of psychotherapy education and training. This should result in a continuous feedback loop between education and training of psychotherapists, empirical evaluation in science and practice, and the reformulation of competence lists as a basis for revising the training curricula for psychotherapists (see figure 1).

How competence profiles, current research and practice, and education inform each other.9
Mechanisms and processes
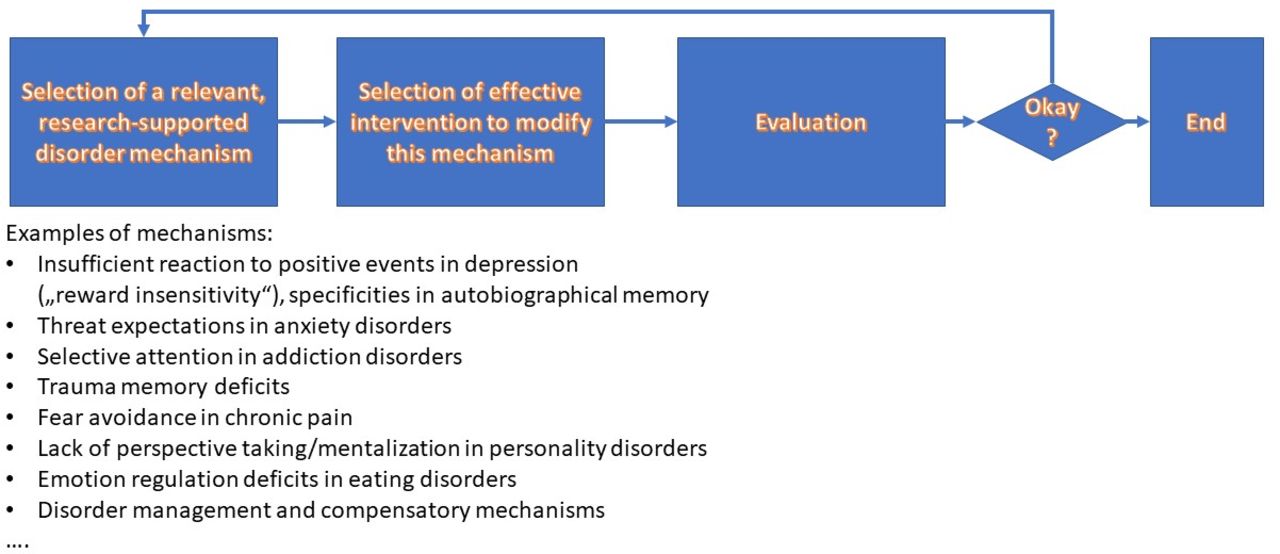
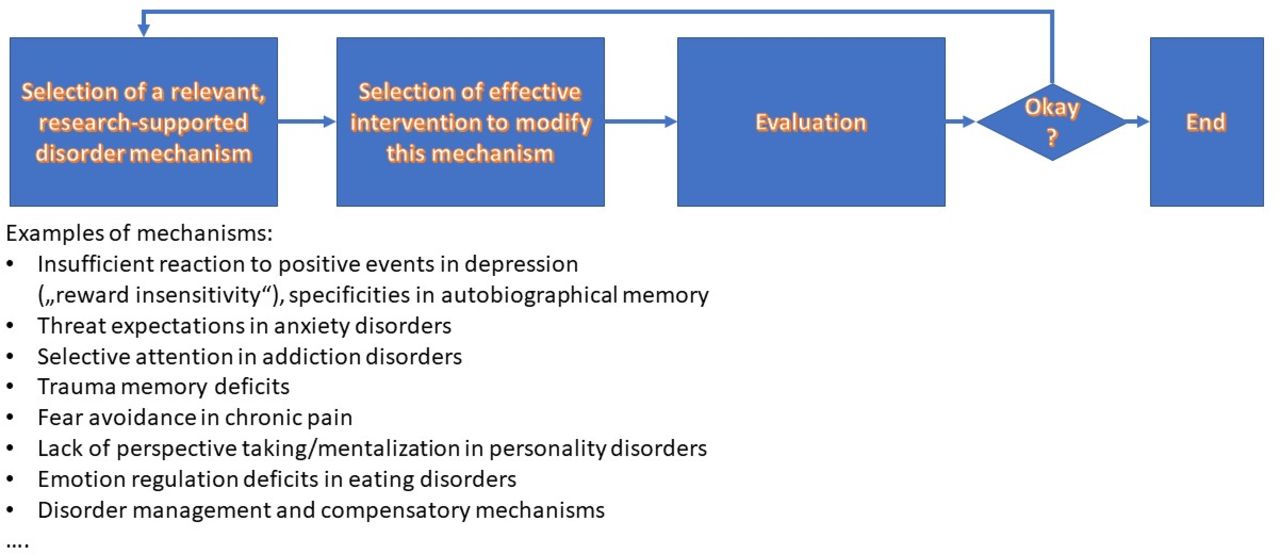
With the introduction of the Research Domain Criteria (RDoC),13 more emphasis was given to psychologically and neurobiologically characterised mechanisms of mental disorders. The knowledge of relevant mechanisms, such as attention and memory processes, predictions/expectations, avoidance, communication/interaction patterns, fears and skills is rapidly increasing. The role of fear avoidance in chronic pain,14 reward insensitivity in depression,15 or trauma and attachment styles in early onset chronic depression16 are specific examples. These processes are not limited to one single theoretical psychotherapy school but are of relevance for understanding mental disorders in general. This leads to the necessity to better characterise the processes of psychotherapy using these general psychological constructs. In this way, the shortcomings of the RDoC should be eliminated (eg, preferences for neurobiological approaches; lack of consideration of patients’ needs).17 Instead of considering psychotherapy as a closed package of one intervention programme, it is understood more as a combination of sequences in the therapeutic processes. Goldfried expresses that ‘moving from theoretical orientation to processes of change’ is necessary.5 Increasing motivation for psychotherapy and for change, exposing oneself to avoided situations, developing new illness beliefs and concepts about change, improving various psychological skills (eg, communications skills, emotion regulation skills, mentalisation skills), reflecting therapeutic and non-therapeutic relationships, and evaluating discrepancies between life goals and present behaviour are just a few examples of these processes. An example of treatments focusing on the therapeutic relationship is given below. Hayes and Hofmann18 identified 18 core processes of cognitive–behavioural therapy (CBT) interventions, but this concept can easily be extended to cover intervention processes of treatments originating from other traditions and frameworks. Evidence-based treatments according to their approach move their focus from evaluating overall treatment packages in large group studies, to mechanisms and processes that are well founded in empirical research (see figure 2). This is also the case for moving from nomothetic (group studies) to idiographic (treatment of one person) approaches.
{kind=link}
{kind=link}
Psychotherapy as a sequence of processes.
The special role of expectations
Emphasising expectations reflects our modern understanding of the brain as a continuously producing prediction-coding organ. Expectations and expectation violation determine our well-being, with expectation violation as the basis for learning.19 Placebo mechanisms confirm that patients’ expectations are major predictors of outcome in most fields of medicine and mental health.20 Most psychological interventions aim to violate existing expectations. Relevant expectations for psychotherapy can be about symptoms (eg, ‘they will persist forever’), coping abilities (‘I will not be able to cope with it’), relationship expectations (‘Eventually, my partner will hurt my feelings again’) and others. Successful psychotherapy typically implies that these disorder-relevant expectations are modified. Actually, this idea was expressed by early psychoanalysts (‘psychotherapy as a correcting experience’),21 but it can be similarly adapted to update the cognitive model of depression (psychotherapy as a tool to change expectations about one’s own experiences and behaviour, expectations about the experiences and behaviours of others and further expectations about future events),22 23 and it fully fits with the current understanding of why exposure therapies are effective.24 25 Therefore, better understanding of how to violate and change expectations is crucial for the improvement of psychological treatments.26
Switching from categorising psychological interventions according to monolithic theoretical frameworks to categorising them according to relevant treatment mechanisms and processes provides an improved framework that respects the common and specific factors of different interventions.
A new categorisation of psychological treatments
An understanding of the relevant subaims and treatment processes helps to better define the interventions and their similarities and differences. As an initial proposal, the following categories are suggested, while being aware that further expert discussions should lead to modifications, reformulations and extensions:
Improving psychological skills
The major idea of this intervention process is that deficits in the relevant psychological skills contribute significantly to vulnerability and the maintenance of mental disorders. Psychological skills such as communication, emotion regulation, perspective taking and mentalisation, improving mindfulness and acceptance strategies can be assessed and specifically targeted in interventions. Many of these interventions have been developed from a CBT background, but the so-called structure focus in some psychodynamic treatments27 and the acceptance part of Acceptance and Commitment Therapy (ACT)28 or mindfulness are further examples. The focus is on learning new behaviour and cognitive strategies that are of relevance to better cope with the challenges of life, symptoms of disorders or to strengthen existing psychological competences.
Relationship-focused psychotherapies
A major assumption of these interventions is that some people with mental disorders have a tendency to establish specific relationship patterns that are dysfunctional in some sense, and that these frequently repeated patterns need to be modified. Attachment theory can offer one theoretical framework for these approaches,29 but other concepts are also available.30 The aetiology of the establishment of these relationship patterns is typically seen in early childhood experiences (eg, relationship with parents in psychoanalysis), but further traumatic experiences or compensation strategies for former negative experiences are also considered (eg, schema therapy).31 The Cognitive–Behavioural Analysis System of Psychotherapy also offers a condensed framework for how to address relationship issues (‘transference hypothesis’),32 as does transference-focused therapy.33 A major characteristic of these interventions is that they use the current therapeutic relationship as an example of how to identify dysfunctional relationship patterns, how to reflect them and how to modify them. Although these interventions have different theoretical backgrounds, they share the same treatment goal.
Clarification of motivation and goal-oriented psychological interventions
For many patients, conflicts or ambivalences between intrinsic goals and extrinsic behaviour or experiences constitute an important part of our understanding of the disorder. To clarify conflicts, nearly all treatment traditions have developed their own procedures, starting from the Rogerian non-directive approach, psychodynamic clarification procedures, pro/con-dialogues in CBT, the chair technique in Gestalt therapy, to more existential treatments and life goal analysis as suggested in ACT. An overarching aim of these treatments is the clarification of motivation and goal-directed behaviour.
Further categories can be added to better classify psychological treatments. This helps to better detect the similarities between interventions, and to improve communication between psychotherapists from different orientations but who share specific goals. Therapists in training should be enabled to switch between these strategies, or integrate them beyond their traditional boundaries. This is not arbitrary eclecticism, but a rational therapist behaviour that is characterised by one and the same goal, and by one mechanism and coherent procedure, ideally being founded in evidence-based mechanisms and processes. The ‘borrowing’ of similar interventions from other therapy traditions that follow the same goal is nothing that should be sanctioned in favour of puristic ideas, but, in contrast, the selection and combination of effective interventions from different theoretical frameworks is a major sign of science, and is often the motor for scientific progress.
This recategorisation of psychological interventions, combined with a better understanding of mechanisms and treatment processes, invites new concepts for training and education in psychotherapy.
The future of training in psychotherapy
A revision of our thinking about training and education in psychotherapy is seriously needed. A major goal is considering the competences that successful psychotherapists really need, and to better focus our training to convey them. At present, the necessary competences can be categorised into the following clusters (box 2):
A scientifically based knowledge about relevant mechanisms and treatment processes. Empirical psychology offers the main contributions (instead of monolithic theories). As the Lancet Psychiatry Commission on psychological treatments summarises, the improvement of links between clinical psychology, psychiatry and basic research offers the potential to deliver more advances in psychological treatments.34
Competences for how to address and modify these mechanisms and processes. Every therapist needs skills to practice the different categories of psychological interventions, such as improving skills and competences of patients, working with therapeutic relationships, and clarifying motivation, short-term goals and life goals.
Developing the necessary personal competences to become a successful psychotherapist. Every successful therapist needs personal competences, that will substantially influence treatment course and outcome. Communication skills, empathy, perspective taking and mentalisation, as well as emotion-regulation skills, are a few examples. Psychotherapy is typically the art of dealing with conflicts, therefore psychotherapists also serve as models for dealing with unexpected problems, showing psychological flexibility and helping to structure problematic situations. Therapists’ expectations are also determinants of treatment course and outcome and thus need to be reflected.
Selection of major fields of competences of psychotherapists to be considered in education and training (short version)
Field
Academic knowledge about mechanisms and processes of mental disorders, psychological factors in medical conditions, processes of change in psychological interventions (not limited to one orientation).
Competence to improve skills of patients (eg, communication, assertive behaviour, emotion regulation and expression, acceptance and tolerance of aversive states, perspective taking and mentalisation).
Competence to work with (therapeutic) relationship: reflection and change.
Competence to clarify conflicts, ambivalences, motivation, (life) goals.
Ability to regulate therapist’s own behaviour, emotions, cognitions, giving priority to the current treatment goals.
Instead of letting people create their own idiosyncratic concepts of how to integrate interventions from different theories, we have to offer a scientific framework for the understanding of disorders and for the planning of different processes of therapies, hereby overcoming the current boundaries of traditions. We have to move forward from evaluating full packages of interventions according to one theoretical framework, to better characterise personalised understanding of problems, to better plan sequences of interventions and to better decide which intervention processes have a high research-based likelihood of leading to treatment success. Good therapists are not those who have perfect knowledge of one theoretical framework, but those who have the competence to use tools to achieve specific goals in specific treatment processes successfully.
If we want to further develop psychotherapy as an academic discipline, we have to discontinue training in very specific techniques or according to one ideology. Research has to be strengthened that leads to decision frameworks when and how to combine interventions from different frameworks, and when and how to adapt psychological treatments if procedures do not lead to the goal of the specific treatment process. Feedback systems can be useful tools to improve interventions, and further evidence-based strategies to adapt ongoing interventions are needed.35 These comments should not be misunderstood as defending unscientific eclecticism, but as a plea to develop more scientific frameworks for treatment decisions that are not bound to one single theory and to be even more scientific and evidence based by reducing the neglect of results that are beyond the favoured theory.
Are current training programmes for psychotherapists really optimised to follow these goals? Serious doubts are warranted. However, if we manage to better define the training goals and competences of psychotherapists, we should be able to optimise our training. Finally, such an optimised way of training young psychotherapists should result in benefits compared with classical training that should be demonstrated in future studies. These types of advantages can be numerous: more economic and effective trainings, better flexibility of psychotherapists, readiness for improved personalised treatment planning and improved outcome at the very end of these revisions.
Conclusions
Current education and training in psychological interventions is often based on the different traditional roots, and this strong identification with specific traditions continuously hinders the scientifically based development of psychotherapy. However, this ‘prescientific stage’6 can be overcome. An important first step is the development of competence lists which are necessary not only for successful treatments, but also for the general requirements that societies and their stakeholders expect from psychologists and psychotherapists. The societal task of this professional group is not just to deliver one single treatment tradition, but also broad expertise and state-of-the-art scientific knowledge of the field.
Many successful psychological interventions are combinations of different treatment processes that are characterised by specific subgoals and a focus on scientifically proven mechanisms. It does not make sense to develop a sixth, seventh or eighth theory framework postulating to be completely different and having some general advantages over the others, but to focus on scientifically evaluated disorder and treatment mechanisms and to steer treatment processes according to these subgoals. This paves the way for psychotherapists to make the best of all the evidence-based expertise that exists for this specific clinical problem. Although this also requires new types of psychotherapy research, the education of psychotherapists has to include all the relevant treatment processes accordingly, so that every psychotherapist is able to offer successful interventions to bring this process to a successful subgoal. Of note, this revision also allows improved integration of modern technical developments supporting psychotherapy.36
Finally, providing successful psychotherapy is always associated with a broad variety of personal competences of psychotherapists. Current approaches to improve these competences in young psychotherapists are either extremely theory loaded, focusing on only a few necessary competences, or overly oriented on academic knowledge. Instead of applying just one theoretical framework that may or may not be effective for the development of the necessary personal skills, a systematic training programme for psychotherapists is needed that directly focuses on the training of their personal competences.
Data availability statement
No data are available. No data included in this manuscript.
Ethics statements
References
Footnotes
Contributors The manuscript was exclusively written by the author.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.