Article Text

Abstract
Background There is an urgent need for context-specific research leading to development of scalable interventions to address self-harm and suicide in low and middle-income countries (LMICs).
Objective The current study was conducted to determine the contents of a psychological intervention to reduce recurrence of self-harm and improve functioning in youth who self-harm in India and finalise its delivery mechanisms.
Methods A systematic, sequential approach was used to integrate available scientific evidence, expert service providers’ knowledge and experience, and service users’ lived experiences in the codesigning and development of a psychological intervention. The steps included: identifying prioritised outcomes for youth who self-harm as well as a selection of feasible and acceptable elements from self-harm interventions that have been trialled in LMICs, intervention development workshops with mental health professionals and youth to finalise elements, a review of relevant treatment manuals to decide on the treatment framework, and finalising the treatment structure and schedule in the second round of intervention development workshops.
Findings We developed ATMAN treatment with three key elements; problem solving, emotion regulation and social network strengthening skills. The delivery schedule emphasises on the engagement elements, and allows for involvement of other stakeholders such as family members when acceptable to the clients.
Conclusion and clinical implications ATMAN treatment could prove to be especially effective in reducing self-harm recurrence in youth in India due to its brief schedule, elements that have been selected in collaboration with the service users and its potential to be scaled up for delivery by non-specialist treatment providers.
- suicide & self-harm
Statistics from Altmetric.com
Introduction
Suicide is a leading cause of premature mortality across the world.1 Low and middle-income countries (LMICs) carry the major burden with three quarters of global suicides occurring in these countries.1 India is home to one-third of global female and one-quarter of global male suicide deaths and suicide is the leading cause of mortality in young people.2 Self-harm (defined as an act of intentionally causing harm to own self, irrespective of the type, motive or suicidal intent) is one of the strongest antecedents of suicide in youth. The risk is higher in 10–24 year-olds as compared with older age groups, and increases with the number of self-harm episodes.3 The risk persists beyond the initial period following self-harm with 1 in 15 dying by suicide after 9 or more years.4
WHO recommends using psychosocial interventions for self-harm to reduce the burden of suicide. Cognitive–behavioural therapy (CBT) and dialectical behaviour therapy have emerged as the most promising interventions to reduce self-harm in adults.5 Although there is limited evidence of effectiveness of psychological interventions in reducing self-harm in children and adolescents, dialectical behaviour therapy for adolescents (DBT-A), mentalisation-based therapy and therapeutic assessment have shown some positive findings.6 Most of the existing studies to evaluate psychotherapeutic measures to reduce self-harm recurrence have been conducted in high-income countries.
Far less attention has been given to develop and evaluate context-specific psychotherapeutic programmes to address this public health crisis in contexts where the implementation of such interventions is likely to encounter a range of supply and demand barriers, such as the lack of mental health specialists and stigma associated with consultation with mental health services.1 There is an urgent need for context-specific research to guide the efforts of service planners, developers and providers in India and other low-resource settings globally to address self-harm and suicide.
There is now a rich body of evidence describing the content and implementation of scalable psychological treatments which are effective when delivered by non-specialist providers in routine care settings in diverse low-resource countries.7 This body of experience has generated valuable knowledge on the critical principles and methods for the design of such interventions. A key principle is the utilisation of non-specialist providers to deliver brief interventions in community and routine care settings, a concept referred to as ‘task-sharing’. However, there is no comparable literature on interventions for persons who self-harm, and this is critically important as self-harm is increasingly recognised as a unique clinical phenotype which is, especially in LMICs, only occasionally associated with a clinically diagnosable mental disorder.8
Guided by this evidence, we describe a systematic, sequential approach to integrate available scientific evidence, expert service providers’ knowledge and experience, and service users’ lived experiences in the codesigning and development of a psychological intervention to reduce recurrence of self-harm and improve functioning in youth with self-harm in India.
Objective
Our overarching objective was to design a scalable intervention which addressed two key questions: what should be its content (eg, the ‘active’ elements); and how should it be delivered (eg, the number of sessions). We anticipated the design of a theoretical map which elaborated the pathways through which the components of the intervention would lead to the desired goals of reducing the recurrence of self-harm and improved functioning.
Method
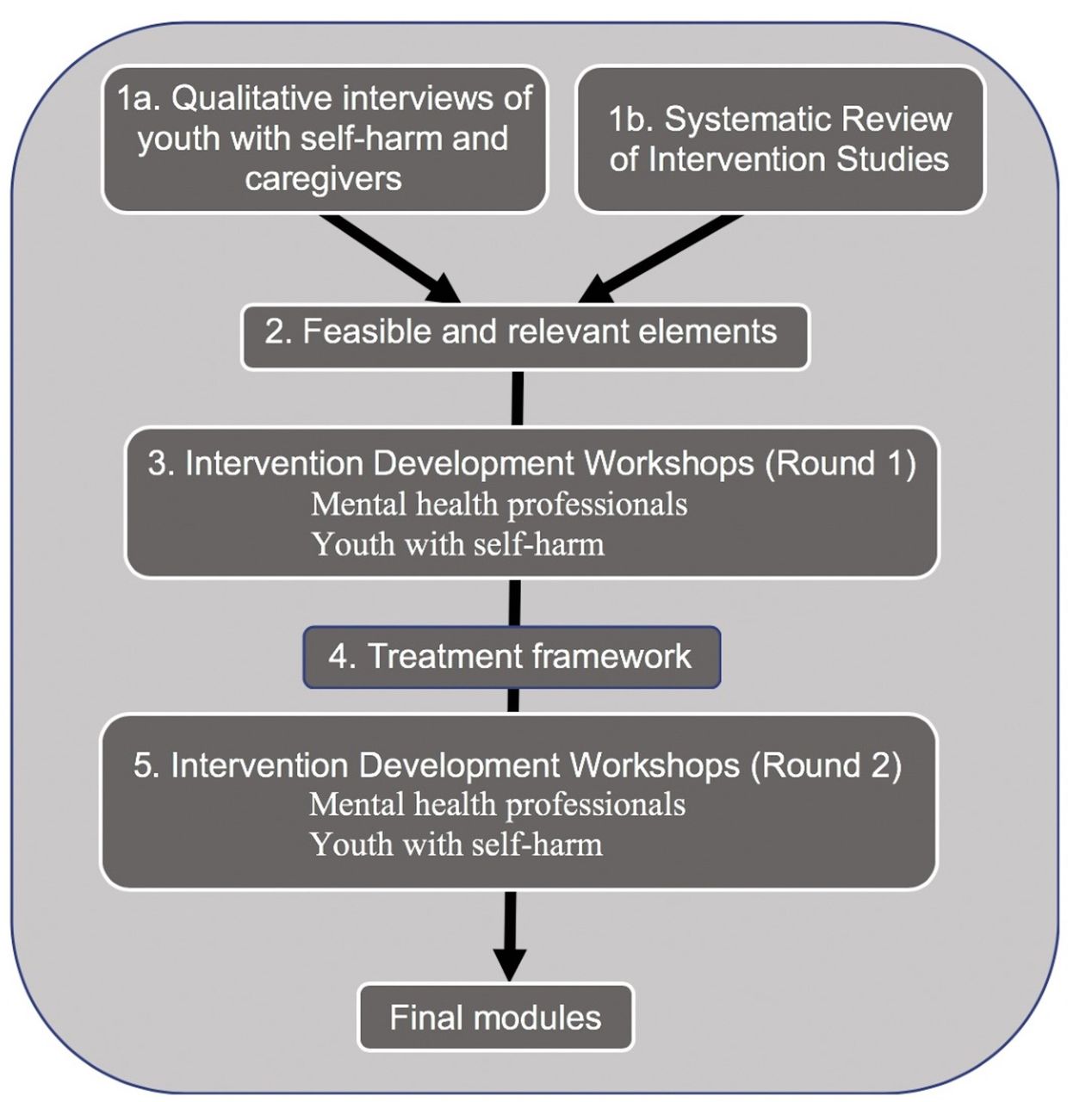
This mixed methods research to develop the intervention consisted of a sequence of studies (figure 1). In the first step, we evaluated the context in which intervention had to be used and identified the prioritised outcomes (‘what matters the most’) for youth who self-harm, and the elements that have been used in self-harm interventions trialled in LMICs. The findings of the in-depth interviews with the youth with self-harm, and their caregivers as well as the systematic review findings (together comprising step 1 of figure 1) have been published elsewhere.9 10 In the next step, a selection of feasible and acceptable elements was identified from the pool of elements identified in step 1. In step 3, the elements for our intervention were finalised during two intervention development workshops: one with the mental health professionals (MHP), and another with the youth with self-harm. A review of relevant treatment manuals followed with the goal of developing a treatment delivery framework in step 4. We finalised the treatment structure and schedule in the second round of intervention development workshops in step 5 (figure 1). The draft treatment emerging was named ATMAN (a Sanskrit word that refers to the ‘eternal self’ that functions in harmony with the Universe) specifically tailored for youth population with self-harm behaviour. A similar stepwise approach has been used successfully to develop two brief psychological treatments for depression and harmful drinking delivered by non-specialist providers to primary care attenders in India.11 12
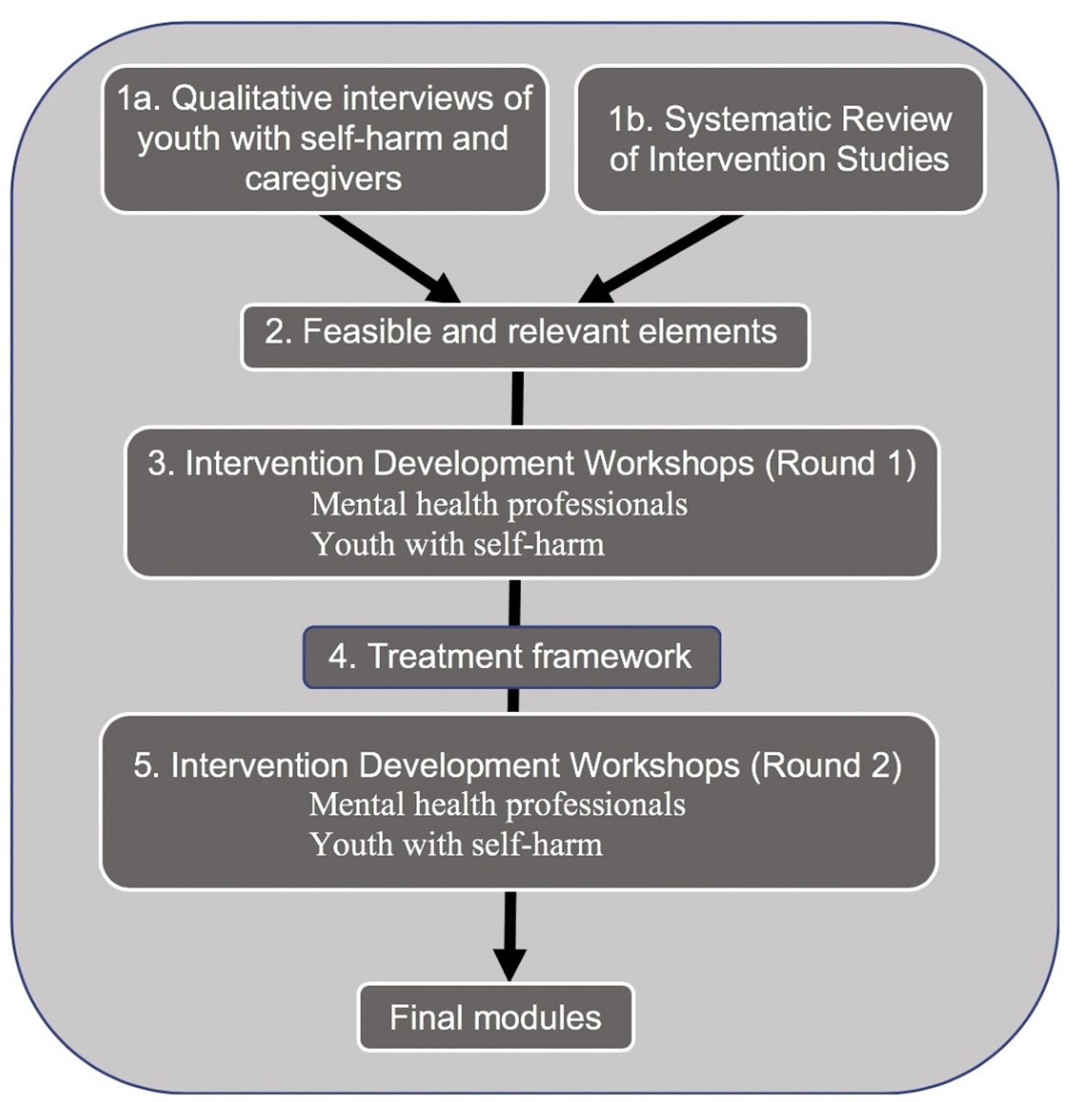
Intervention development process of ATMAN.
Details of methods and findings
The research steps described in the paper occurred between July 2018 until December 2019 and were conducted in Mumbai. For the ease of understanding, we have outlined the details of the methods used and the findings of each step together.
Step 1: Context evaluation and identifying potential elements from literature
We conducted 15 in-depth qualitative interviews with youth (from 15 to 24 years of age) and four interviews with the caregivers of youth presenting to the psychiatry department of a major public sector tertiary hospital located in Mumbai, India following a self-harm attempt (online supplemental appendix 1). The interviews evaluated the individual experiences and perspectives of youth and family members around self-harm as well as the range of psychopathology to inform the design of the intervention.9 The recorded and transcribed interviews were analysed using phenomenological thematic analysis. The subthemes were identified to capture the essential qualities of the interviews and those with a common point of reference were unified into themes. During the process, we were able to define and prioritise the outcomes that should be addressed by the intervention and assessed in the evaluation of its impact: conflict resolution skills; emotional regulation skills; and social network strengthening skills.9
Supplemental material
Separately, we conducted a systematic review of the evidence on the acceptability and effectiveness of psychological treatments for self-harm that have been trialled in LMICs. Distillation techniques were used to identify effective ‘elements’ in the interventions used in the studies. An element was defined as a therapeutic activity or strategy.13 This method helped us in identifying 27 treatment elements including both self-harm specific and generic elements (table 1). Furthermore, the review helped us in identifying barriers in effective treatment for self-harm in youth in an LMIC setting, and a corresponding intervention delivery model to ensure more efficient targeting using limited resources.10
Stagewise selection of intervention elements
Step 2: Selection of feasible and acceptable elements
In this step, we selected the elements likely to be acceptable and feasible by matching the characteristics and needs of youth who self-harm with that of participant characteristics in the published studies.9 10 The characteristics included age and gender. The needs were assessed by the dimensions of psychopathology as well as contextual factors related to self-harm reported by the service-seeking sample.9 Each element identified in the previous step was evaluated for inclusion in the intervention. As a result, 15 evidence-based elements were selected (table 1).
Step 3: Intervention development workshops to finalise intervention elements
We conducted intervention development workshops with the goal of finalising the selection of treatment elements, by identifying missing elements and elements which were unlikely to be scalable either due to lack of feasibility of delivery by non-specialist providers or acceptability for the patient population. We conducted one workshop each with two key stakeholders of the proposed intervention: MHPs and youth who self-harm. Both the workshops were facilitated by the first author (SA). It was explained to the participants, both in the information sheets and at the start of the group discussion, that they would not be asked any personal or sensitive information during the workshop and they could share what they felt comfortable with.
During the workshop, treatment elements identified from previous steps were introduced to the participants. They were encouraged to reflect on their experiences, and share it with the group. This was followed by a consultation in order to identify which of the elements would be acceptable by self-harm clients in the Indian context and were feasible for delivery by counsellors. A handout with the shortlisted elements was given to each participant for rating on a five-point Likert scale on four dimensions: feasibility (is it possible for non-specialist providers to deliver this element with appropriate training and supervision); acceptability (is the element suitable for the Indian cultural context and most common circumstances); effectiveness (does the element bring an important and positive change in the self-harm behaviour); and risk of harm (is there any risk involved in a non-specialist provider delivering this element). Additionally, participants could add any element they felt was missing and essential. Mean scores of findings of both sets of participants were used to rank the elements (elements with an overall score of 3.5 and above on the five-point Likert scale were retained) which were to be taken forward to the next step of the intervention development process. The findings were recorded on a flip chart. Additionally, the discussion was audio recorded and was transcribed verbatim for analysis of content. The analysis of the transcribed discussion was carried out using thematic analysis. The first author and the field worker independently coded the transcripts after familiarising themselves with the data, noting observations and descriptive comments to reach an initial understanding of the content. The subthemes were identified from the data to capture the essential qualities of the discussion and subthemes with a common point of reference were unified under the respective elements (table 1).
Mental health professionals
Three psychologists, one social worker and one senior psychiatrist working with youth with self-harm participated in the professionals’ intervention development workshop. We purposively selected the professionals to represent different settings, experience levels and disciplines (online supplemental appendix 1). For example, the psychiatrist had over 30 years of experience in the field and had been heading the department of psychiatry in a tertiary-level public hospital in Mumbai for two decades. The department has around 250 clients in its outpatient clinic every day, of which approximately 40% consist of children and adolescents.14 On the other hand, another participant was a clinical psychologist with a recent start in a private setting. We included her to get a perspective of someone closer in age to the clients for whom the intervention was being designed and with a recent training experience.15
Youth with self-harm
Six participants aged 15–24 years who had presented to the tertiary hospital emergency department following a self-harm attempt were recruited. In this intervention development workshop, the understanding, perceptions and opinions of the participants on treatment elements and what is likely to work to reduce the recurrence of self-harm were explored, with a particular focus on their previous experience with treatment, and barriers to implementation of any of the elements.
Findings
The professionals mentioned factors such as communication difficulties, parenting difficulties, support needs of parents and problems related to managing expectations of others as the key targets that the intervention elements should address to reduce the recurrence of self-harm. Both groups mentioned factors such as difficulty in managing intense emotions, low self-esteem and self-worth, low frustration tolerance, limited coping skills and psychopathology such as depression and anxiety as potential targets (table 2).
Intervention development workshop findings
Very often parents are not open to communication, to accept that there is something going on with their child and they don’t even ask ‘how was your day’ or ‘is there anything you need help with’. It is easier for young people to talk to and open to their friends. (MHP on communication between parents and youth)
Important treatment-related themes from professionals’ intervention development workshop helped us in identifying suitable elements. The inputs included increasing insight into the problem leading to greater motivation to change resulting in better outcomes; requirement of any treatment to be developmentally appropriate; involvement of the family in treatment in a manner acceptable to them; making the treatment process structured and easy to understand; addressing the difficulty young people experienced in discussing self-harm with their parents; and the role of the friends which was more prominent and supportive.
They feel what they (youth with self-harm thoughts) are thinking is rubbish. There is an extreme sense of shame which comes with it. How can I harm myself, especially cutting. (MHP on need of psychoeducation)
If they are motivated it results in better outcomes. And I think self-referral is actually a very critical aspect, because self-referral means I am trying to figure out how not to do this. (MHP on motivation to change and outcomes)
Important themes that emerged in youth workshop were the need of the treatment providers to be empathic, to involve family members in the therapy process and to address stigma related to treatment.
No one had any time…Counsellor asked a few things, doctor just gave me medicines. I felt so bad when I went back home. I felt what was that…. (Youth on their treatment experience following self-harm)
If the girl has harmed herself, is it not important to involve her husband who might be responsible for her self-harm…everybody gets busy trying to tell the girl what she did was wrong and she should try to change herself. (Youth on the need to involve family members)
People say, she has gone crazy, mad. That’s why she is going to see the doctor… they taunt. (Youth on the need to address stigma related to treatment for self-harm)
During this set of workshops, we identified 14 elements from the list (table 1) which met our a priori cut-off of a combined average score of 3.5. Motivational enhancement for substance use where useful was proposed during the MHPs’ workshop and was added to the list of elements. Relaxation strategies and relapse prevention were eliminated due to low scores.
Step 4: developing a treatment framework
We analysed the contents of relevant treatment manuals for young people who self-harm during this step. Our goal was to assess the suitability of any of the existing manuals to be used as a primary manual and the extent to which adaptations would be required. We evaluated the adequacy of implementation of elements identified through our formative research and their sequencing. We initially reviewed the C-MAP manual, a problem-solving therapy for suicidal behaviour adapted and evaluated in Pakistan due to similarities in the sociocultural context.16 However, as this manual is not specific to youth, we also referred to three other manuals which included elements that were identified and had been specifically designed for young people with self-harm and/or mental health problems. These included a CBT workbook for treating self-harm in young people (Cutting Down)17; ASSIP, a brief therapy based on a patient-centred model of suicidal behaviour with an emphasis on early therapeutic alliance18; and the transdiagnostic brief problem-solving intervention manual designed and evaluated in a school-based adolescent population in India.19
A review of these manuals and protocols helped us to identify ways to incorporate the 14 elements in a modular intervention and finalise the delivery rules.16–19 We formulated the treatment to consist of three modules with three additional optional modules. Each module consisted of a meaningful unit, which could bring about a specific treatment outcome.20 The three modules were problem solving and crisis management; emotion regulation; and social network strengthening (table 3).
List of modules and elements finalised in step 4
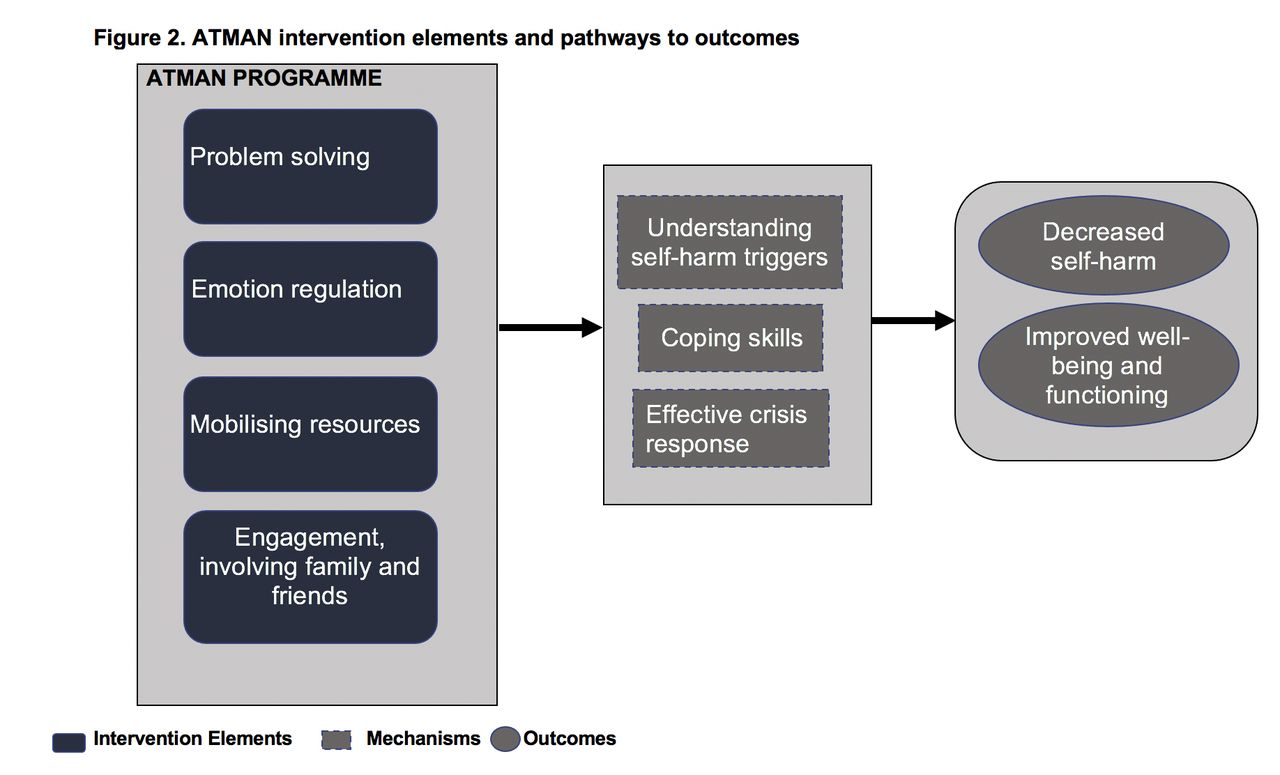
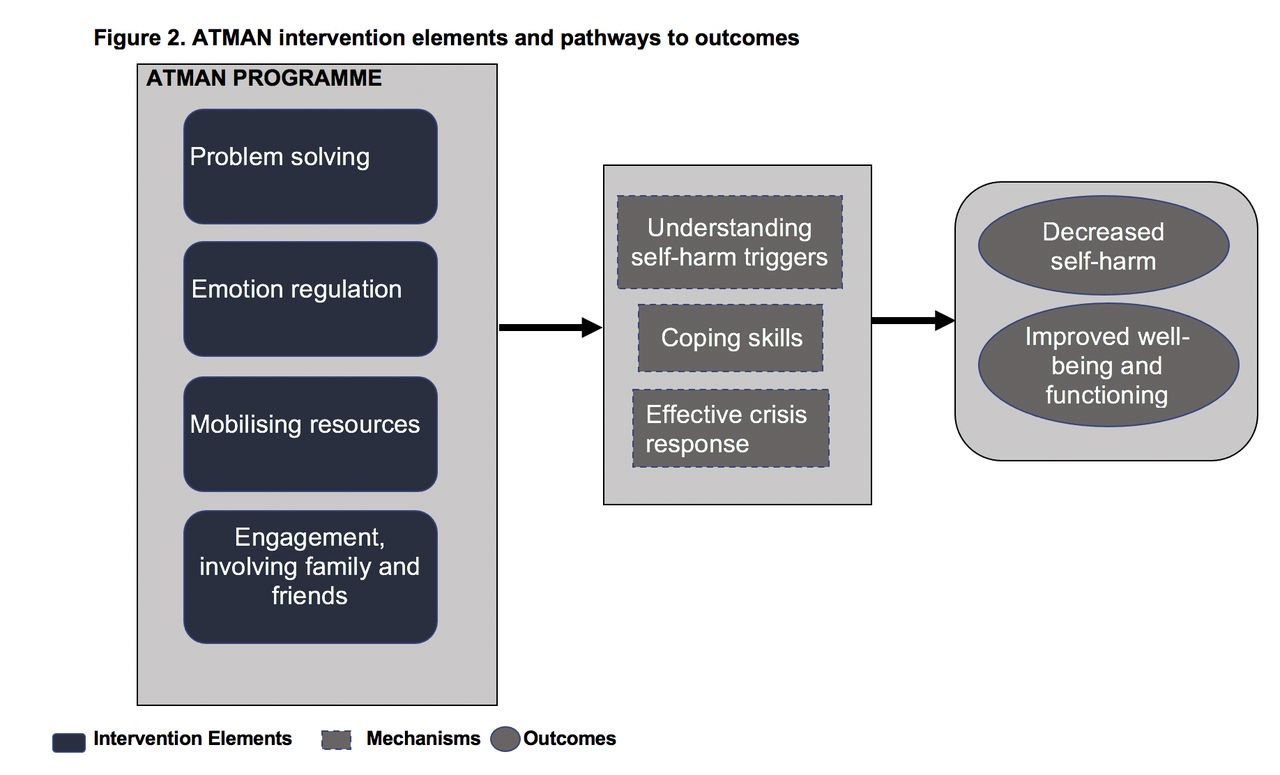
Three additional modules included a family module; substance use; and the assertiveness skills training module which could be used at the discretion of a counsellor, if deemed appropriate. The family module was kept optional to give young people a choice about the involvement of the family in their treatment leading to a greater control and trust in the process. The mechanisms by which the final intervention elements could lead to the desired outcomes were hypothesised as improved coping skills, understanding the self-harm triggers for an effective response and better management of the crisis situations (figure 2).5 6 21 The emerging ATMAN manual included contextually appropriate treatment elements; was easy to understand for non-specialist providers; and comprised age-appropriate and culturally relevant case vignettes and scripts.
{kind=link}
{kind=link}
ATMAN intervention elements and pathways to outcomes.
Step 5: finalising the treatment structure
This final step involved two intervention development workshops: one with the youth with self-harm and with MHPs to guide the intervention schedule, sequencing of modules and finalising the treatment structure. Intervention materials suitable for psychoeducation of clients and a step-by-step guidance manual for use by counsellors were the deliverables of this step.
The workshop with the MHPs comprised five professionals consisting of a college counsellor, school counsellor and three psychologists working in the private sector. All six participants of the youth intervention development workshop in step 3 were invited; four participants who had participated earlier were able to join the workshop along with three new participants (online supplemental appendices 2 and 3).
Based on recommendations from the second round of intervention development workshops, modifications were made to contents of the modules: self-soothing element was moved to problem solving and crisis management module; and distraction strategies were shifted to emotion regulation module. Additionally, family psychoeducation that was earlier part of the social network strengthening module was moved to problem solving and crisis management module.
I think it is important to have the family members present when people are trying to make me understand the reasons for my current state. I was tired with the counselling that I got after I harmed myself without anyone talking to my husband, who was my biggest problem. (Youth)
Psychoeducation should involve the family members as many of them are highly stressed and don’t know how best to support the client. There is a lot of shame, guilt and hostility seen in such situations. (MHP)
Youth can be given the option of whether they would like to involve the family members in the first session. I feel there could be some provision of involving friends at some stage as they act as better support system for youth who self-harm. (MHP)
I think self-soothing strategies that youth have used and found helpful should be clubbed with crisis plan as a reminder of things they can do during the most difficult times. (MHP)
Discussion
This paper describes the inception and evolution of an intervention for self-harm in youth in India. We used a systematic methodology integrating the local and global evidence, that is, acceptable to young people in the context of its delivery and deliverable by non-specialist providers. There were a few key reasons for us to select problem solving, emotion regulation skills and mobilising social support as the key elements for the intervention. They include: the findings from the in-depth qualitative interviews and intervention development workshops showing a range of problems best addressed by these elements; promising results shown by problem-solving therapy in the systematic review of randomised controlled trials in the community for self-harm in children, adolescents and adults5 6; evidence showing deficient social problem-solving skills in people with self-harm with a greater reliance on others and a passive approach to problem solving22; emotion regulation skills and increasing family support as important elements of the interventions with effects in reducing self-harm in adolescents21; and limited access to emotion regulation strategies significantly predicting suicidal ideation.23 Furthermore, problem solving with integrated behavioural activation and social support strengthening are the key elements in intervention for training lay workers to address depression, anxiety and stress in communities affected by adversities endorsed by WHO.24
There is limited empirical evidence for the effectiveness of psychological interventions in youth self-harm. Although these findings need further replication, emotional clarity, and having access to effective strategies to respond to and recover from emotional dysregulation are two dimensions of emotion regulation that are linked to suicide risk.25 We identified emotion regulation as an important element for our intervention from the formative studies.
The third key element of the ATMAN intervention programme is social network strengthening. Limited social networks are associated with self-harm with enhancement in social network possibly offering some protection against self-harm.22 Social network strengthening strategies can be an important element in self-harm management especially in Asian context.26 Our formative studies highlighted the importance of peer groups and family members in the management of self-harm. In addition, a sense of social isolation due to an absence of a network outside the family, especially in females, was an important theme that emerged from the in-depth interviews of youth with self-harm.9
The formative studies highlighted the importance of engagement elements and crisis planning. The counselling experiences of participants explored during the in-depth interviews showed the importance of rapport, and shared goal setting for any intervention to be acceptable and useful. The participants felt the counsellor was keener to give advice rather than listening to them, understand their experiences and work on a collaborative plan. This finding is substantiated by research showing the importance of engagement elements in any successful psychotherapeutic process. In particular, the therapeutic relationship which is a key determinant of engagement, along with therapeutic alliance, has consistently been identified as positively associated with treatment outcomes.27 The crisis plan, on the other hand, an element relevant for self-harm, was useful in identifying practical support options and problem solving during difficult times. It is part of the standardised guidelines and interventions for management of self-harm.16 18
There are very few psychological interventions for self-harm that have been tested for effectiveness in LMICs.5 None of these have been indigenously developed taking into account client’s unique cultural values and norms while addressing social and individual determinants for youth. Additionally, very few studies have evaluated the effectiveness of psychological interventions in self-harm in children and adolescents. The interventions that have shown promise in reducing self-harm in adolescents globally, such as mentalisation-based therapy and dialectical behaviour therapy for adolescents, involve a core component of intensive, one-on-one extended contact.6 Such intensive treatments with prolonged contact are not feasible in the current study setting due to limited infrastructure, expertise and nature of the presentations which are mostly in the context of situational crisis with limited motivation to engage with the services, once the crisis resolves.9
We developed a framework for intervention suitable to be delivered by the counsellors with adequate training and under supervision. Non-specialist counsellor-delivered interventions have shown to be successful in conditions such as depression and substance use.11 12 We hope to use similar delivery methods for the ATMAN trial and use the findings of the formative studies to optimise the process. The important learnings and deliverables during the process were: (1) the identification of problem solving, emotion regulation and social network strengthening elements that could cater to the range of problems observed; (2) the reformulation of common presentations, strategies that help and barriers in effective treatment for self-harm in youth in an LMIC setting, and corresponding intervention delivery model to ensure more efficient targeting using limited resources; (3) designing of intervention materials suitable for psychoeducation of clients and a step-by-step guidance manual for use by counsellors; (4) a delivery schedule that gives importance to engagement elements and therapeutic relationship, involves other stakeholders such as family members when acceptable to the clients and addresses the challenges considered important by the clients. To overcome some of the limitations such as generalisability that the qualitative research sampling approaches used in formative studies posed, we tried to include a diverse range of participants from various backgrounds for the professionals’ focused group discussions. Similarly, for youth group discussions, we attempted to ensure that the sample was representative of self-harm presentations to a public sector hospital.
Clinical implications
We described the intervention development process for a scalable psychological intervention in youth self-harm appropriate for use in LMICs. There is a dearth of LMIC-based psychological intervention adaptations and studies that provide detailed descriptions of intervention elements for self-harm. By reporting the process and the findings, we hope that similar methodology can be used for local adaptations of ATMAN treatment in other LMICs to address this public health challenge.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SA was involved in conceptualising and designing the study, analysis and drafting the manuscript. GP was involved in designing the study, analysis and drafting the manuscript. MB and VP were involved in guiding the study design, analysis and drafting the manuscript.
Funding This work was supported by the Wellcome Trust-India Alliance Research Fellowship awarded to the first author (grant number IA/CPHE/16/1/502664).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was reviewed and approved by two ethics committees: Institutional Ethics Committee of Lokmanya Tilak Municipal Medical College and General Hospital, Mumbai (IEC/684118) and Institutional Ethics Committee of Public Health Foundation of India, Gurgaon, Haryana (IEC-366/17).
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.